
Rationale and Objectives
The purpose of this study was to quantify the degree of imaging–histologic discordance in a cohort of patients undergoing computed tomography (CT)–guided lung biopsy for focal lung disease.
Materials and Methods
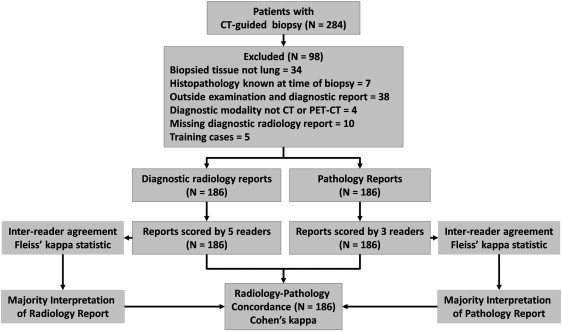
A retrospective review was performed of 186 patients who underwent percutaneous lung biopsy of a parenchymal lesion at our institution between January and December 2009. Diagnostic radiology reports of CT or positron emission tomography–CTs performed before biopsy were used to classify the lesion as malignant or benign by five readers. Pathology reports of the biopsied lesions were classified by three readers. Inter-reader agreement and imaging–histologic concordance were quantified using kappa statistics. Discordant benign cases were then revisited to determine downstream effects.
Results
Inter-reader agreement on report content was substantial or almost perfect with kappas >0.783. Kappas for concordance were as follows: malignant (0.448), primary lung cancer (0.517), metastatic disease to lung (0.449), benign (0.510), and overall agreement (0.381). Of the twelve discordant benign cases that were revisited, four were found to be false negatives, resulting in a delay in diagnosis.
Conclusions
Our study of imaging–histologic discordance in percutaneous biopsy of lung lesions supports the need for imaging report standardization and improved integration and communication between the fields of radiology and pathology.
Radiology and pathology play central roles in cancer diagnosis but typically report findings independently of one another. Independent reporting can increase radiologic–pathologic discordance, defined as a discrepancy between imaging interpretation and histologic findings . Radiologic–pathologic correlation has been studied in various imaging specialties to gauge interpretive performance and accuracy, and to identify radiographic features corresponding to histologic findings . However, few studies have attempted to assess the utility of integrated radiologic–pathologic correlation for establishing imaging–histologic concordance or discordance as a method to prospectively identify missed carcinomas due to biopsy sampling error .
Radiologic–pathologic discordance may be categorized as either discordant malignant or discordant benign. The former refers to a lesion that appears radiologically benign, but is malignant on histology; the latter refers to a lesion suspicious for malignancy on imaging but benign histologically . In mammography, with the adoption of the Breast Imaging-Reporting and Data System (BI-RADS), this notion of discordance fits naturally due to strict, unambiguous radiologic guidelines governing diagnostic conclusions. BI-RADS provides a framework that allows instances of discordance to receive special consideration such that ostensibly negative pathology in cases of high radiographic suspicion warrant prompt repeat biopsy .
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Materials and methods
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Inter-reader Agreement on Interpretation Content
Get Radiology Tree app to read full this article<
Table 1
Sample Reader Scoring of Radiology and Pathology Diagnostic Interpretations
Original Semantic Reports Reader Interpretation of Report Malignant Primary Lung Cancer Metastatic Disease Benign Disease Radiology impression: focal nodule in the right lower lobe with central necrosis. Primary consideration is malignant disease, in particular primary lung cancer or metastatic disease. 1 1 1 0
Get Radiology Tree app to read full this article<
0 0 0 1
“1” indicates that the diagnosis was included as a possible etiology of the lesion of interest; “0” indicates that the diagnosis was not included.
Table 2
Inter-reader Agreement on Information Content of Diagnostic Imaging and Pathology Reports
Radiology Classification Agreement between Readers Fleiss Kappa ∗ Pathology Classification Agreement between Readers Fleiss Kappa ∗ Radiology–malignant, not otherwise specified 0.783 Pathology–malignant, not otherwise specified 0.974 Radiology–primary lung cancer 0.904 Pathology–primary lung cancer 0.964 Radiology–metastatic disease to the lung 0.849 Pathology–metastatic disease to the lung 0.926 Radiology–benign 0.915 Pathology–benign disease 0.972 Radiology–combined 0.817 Pathology–combined 0.925
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Radiologic–Pathologic Concordance
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 3
Cohen Kappa Scores Comparing the Majority of Radiology Diagnosis with Majority of Pathology Diagnosis
Disease Category Cohen Kappa Coefficient between Radiology and Pathology Diagnoses Malignant, not otherwise specified 0.448 (0.304–0.592) Primary lung cancer 0.517 (0.396–0.638) Metastatic disease to the lung 0.449 (0.315–0.583) Benign process 0.510 (0.374–0.647) Combined 0.381 (0.300–0.461)
Get Radiology Tree app to read full this article<
Results
Inter-reader Agreement on Report Content
Get Radiology Tree app to read full this article<
Table 4
Frequencies and Percentages of Conclusions Observed on Radiology and Pathology Reports
Radiology or Pathology Report Description Radiology Pathology_n_ %n % Definitively malignant or benign Malignant, not otherwise specified 15 8.1 0 0.0 Primary lung cancer 55 29.6 81 43.5 Metastatic disease to the lung 45 24.2 38 20.4 Benign process 25 13.4 48 25.8 Primary lung cancer or metastatic disease 1 8 4.3 13 7.0 Ambiguous (malignant or benign) Primary lung cancer or metastatic disease or benign process 5 2.7 0 0.0 Primary lung cancer or benign process 8 4.3 0 0.0 Metastatic disease or benign process 12 6.5 0 0.0 Malignant, not otherwise specified or benign process 6 3.2 0 0.0 Nondiagnostic Indeterminate 7 3.8 6 3.2 Total 186 100.0 186 100.0
Data are based on the majority interpretation by readers for the imaging and pathology reports.
1 Cases in which neither benign nor malignant disease were included in the imaging diagnosis.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Concordance between Radiology and Pathology Reports
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 5
Relationships between Benign and Malignant Pathologic Diagnosis and Radiologic Report
Pathologic Truth ( n = 180) Categories of Radiology Interpretation, n (%) Pathologic Diagnosis, n (%) Malignant Only Benign Only Malignant or Benign Neither ∗ Malignant = 132 (71) 108 (82) 4 (3) 17 (13) 3 (2) Benign = 48 (26) 12 (24) 20 (42) 14 (30) 2 (4)
In six cases (3%), there was insufficient tissue for pathologic diagnosis; these cases are not included.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Outcomes in Discordant Benign Cases
Get Radiology Tree app to read full this article<
Table 6
Features of Cases with Benign Discordance (Radiographic Malignant Diagnosis with Benign Histology)
n Age (years) Sex Radiologic Diagnosis Pathologic Diagnosis Final Diagnosis and Mode of Diagnosis 1 74 M Metastatic colon cancer Hepatic parenchymal sampling Metastatic colon carcinoma, repeat biopsy 3 months later 2 70 M Metastatic thyroid cancer Alveolar tissue with nonspecific fibrosis and chronic inflammation with focus of granulomatous inflammation Metastatic thyroid carcinoma, repeat imaging 2 months later 3 81 M Metastatic sarcoma Lymphoplasmacytic infiltrate Metastatic sarcoma, repeat imaging 5 months later, repeat biopsy 12 months later 4 65 M Metastatic adenoid cystic carcinoma Benign alveolar tissue with focal fibrosis Metastatic adenoid cystic carcinoma, repeat imaging 3.5 months later 5 73 M Metastatic squamous cell carcinoma Amyloidoma Amyloidosis 6 58 F Primary lung cancer Necrotizing granulomatous inflammation, coccidioidomycosis Disseminated coccidioidomycosis 7 48 M Primary lung cancer Pulmonary hamartoma Hamartoma 8 75 F Primary lung neoplasm Necrotizing granuloma, coccidioidomycosis Granuloma 9 51 M Primary lung neoplasm Necrotizing granuloma, likely coccidioidomycosis Granulomatous disease, clinical diagnosis 10 55 F Metastatic breast cancer Fragments of bronchioalveolar tissue and mucin with eosinophils Inflammatory, surgical biopsy 1 month later 11 46 M Primary lung neoplasm Lung with hemosiderin-laden macrophages, mild chronic inflammation Indeterminate, lost to follow-up 12 51 F Malignant, not otherwise specified Benign tissue with focal fibroelastosis, old hemorrhage, rare refractile, nonpolarizable foreign material Lost to follow-up
F, female; M, male.
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Conclusions
Get Radiology Tree app to read full this article<
Supplementary Data
Get Radiology Tree app to read full this article<
Supplementary Appendix 1
Get Radiology Tree app to read full this article<
References
1. Sorace J., Aberle D.R., Elimama D., et. al.: Integrating pathology and radiology disciplines: an emerging opportunity?. BMC Med 2012; 10: pp. 100.
2. Koo H.J., Choi H.J., Kim M., et. al.: Radiologic–pathologic correlation of renal cell carcinoma associated with Xp11. 2 translocation. Acta Radiol 2013; 54: pp. 827-834.
3. Kuriyama K., Tateishi R., Doi O., et. al.: CT-pathologic correlation in small peripheral lung cancers. AJR Am J Roentgenol 1987; 149: pp. 1139-1143.
4. Varma D.G., Ayala A.G., Carrasco C.H., et. al.: Chondrosarcoma: MR imaging with pathologic correlation. Radiographics 1992; 12: pp. 687-704.
5. Bhartia B., Ward J., Guthrie J.A., et. al.: Hepatocellular carcinoma in cirrhotic livers: double-contrast thin-section MR imaging with pathologic correlation of explanted tissue. AJR Am J Roentgenol 2003; 180: pp. 577-584.
6. Lee K.S., Im J.G., Choe K.O., et. al.: CT findings in benign fibrous mesothelioma of the pleura: pathologic correlation in nine patients. AJR Am J Roentgenol 1992; 158: pp. 983-986.
7. Maetani Y., Itoh K., Egawa H., et. al.: benign hepatic nodules in Budd–Chiari syndrome: radiologic–pathologic correlation with emphasis on the central scar. AJR Am J Roentgenol 2002; 178: pp. 869-875.
8. Atkins K.A., Cohen M.A., Nicholson B., et. al.: Atypical lobular hyperplasia and lobular carcinoma in situ at core breast biopsy: use of careful radiologic–pathologic correlation to recommend excision or observation. Radiology 2013; 269: pp. 340-347.
9. Parikh J., Tickman R.: Image-guided tissue sampling: where radiology meets pathology. Breast J 2005; 11: pp. 403-409.
10. Liberman L., Drotman M., Morris E.A., et. al.: Imaging–histologic discordance at percutaneous breast biopsy. Cancer 2000; 89: pp. 2538-2546.
11. Lee J.M., Kaplan J.B., Murray M.P., et. al.: Imaging–histologic discordance at MRI-guided 9-gauge vacuum-assisted breast biopsy. AJR Am J Roentgenol 2007; 189: pp. 852-859.
12. Liberman L., Dershaw D.D., Glassman J.R., et. al.: Analysis of cancers not diagnosed at stereotactic core breast biopsy. Radiology 1997; 203: pp. 151-157.
13. Dillon M.F., Hill A.D.K., Quinn C.M., et. al.: The accuracy of ultrasound, stereotactic, and clinical core biopsies in the diagnosis of breast cancer, with an analysis of false-negative cases. Ann Surg 2005; 242: pp. 701.
14. Youk J.H., Kim E.K., Kim M.J., et. al.: Missed breast cancers at US-guided core needle biopsy: how to reduce them. Radiographics 2007; 27: pp. 79-94.
15. Sobel J.L., Pearson M.L., Gross K., et. al.: Information content and clarity of radiologists’ reports for chest radiography. Acad Radiol 1996; 3: pp. 709-717.
16. Berlin L.: Pitfalls of the vague radiology report. AJR Am J Roentgenol 2000; 174: pp. 1511-1518.
17. (2010) The Importance of Radiology and Pathology Communication in the Diagnosis and Staging of Cancer: Mammography as a Case Study.
18. Team, R.D.C: R: a language and environment for statistical computing.2008.R Foundation for Statistical ComputingVienna, Austria
19. Kundel H.L., Polansky M.: Measurement of observer agreement. Radiology 2003; 228: pp. 303-308.
20. Enzmann D.R.: Radiology’s value chain. Radiology 2012; 263: pp. 243-252.
21. Lee J.K.: Quality—a radiology imperative: interpretation accuracy and pertinence. J Am Coll Radiol 2007; 4: pp. 162-165.
22. Tot T., Gere M.: Radiological–pathological correlation in diagnosing breast carcinoma: the role of pathology in the multimodality era. Pathol Oncol Res 2008; 14: pp. 173-178.
23. Khorasani R., Bates D.W., Teeger S., et. al.: Is terminology used effectively to convey diagnostic certainty in radiology reports?. Acad Radiol 2003; 10: pp. 685-688.