
Rationale and Objectives
The purposes of this study were to provide a case-based overview of various immune-mediated side effects detected by 18F-Fluorodeoxyglucose (F-18 FDG) positron emission tomography-computed tomography (PET-CT) in the patients receiving ipilimumab immunotherapy for treatment of malignant melanoma, and discuss the importance of recognizing immune-mediated side effects in the use of F-18 FDG PET-CT for monitoring therapeutic effects of ipilimumab on metastatic melanoma.
Materials and Methods
This is a retrospective case series study of the patients diagnosed with melanoma who were subjected to immunomodulating therapy with ipilimumab. F-18 FDG PET-CT findings were reviewed, and the patients with immune-mediated side effects were selected for further analysis, in conjunction with review of clinical progress notes, the results of laboratory tests, and findings of other imaging tests.
Results
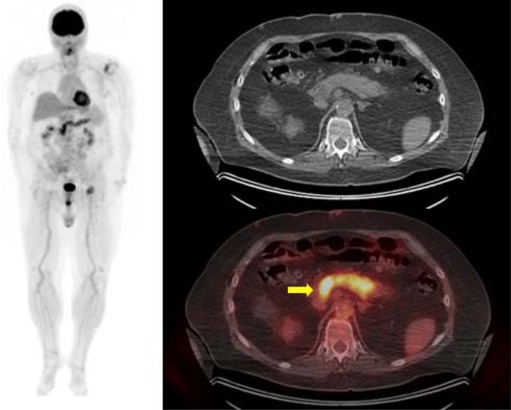
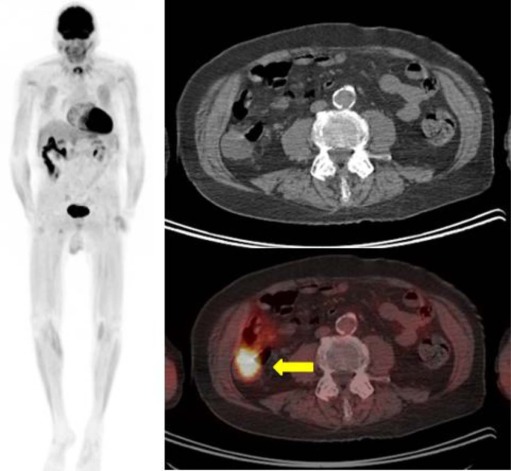
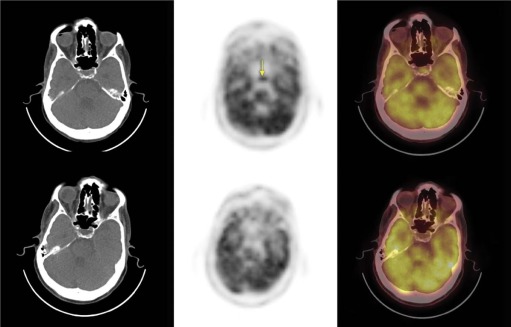
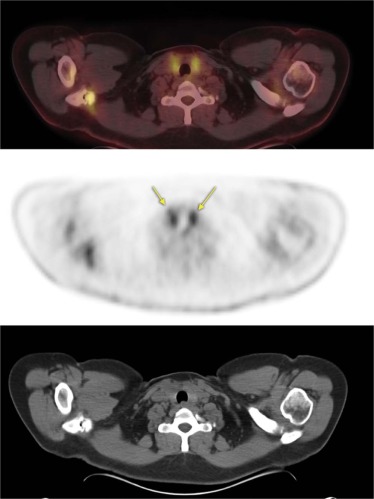
Four patients with immune-mediated side effects were identified among the patients being treated with ipilimumab and subjected to F-18 FDG PET-CT for monitoring therapeutic effects. These immune mediated side effects include new findings of abnormal increased FDG uptake associated with immune-mediated pancreatitis and hypophysitis, as well as immune-mediated thyroiditis and colitis reported previously.
Conclusions
Various immune-mediated side effects were detected by F-18 FDG PET-CT in the patients subjected to immunomodulating therapy with ipilimumab. It is essential for the interpreting provider to recognize and differentiate abnormal FDG uptake associated with immune-mediated side effects from hypermetabolic malignant lesions when using F-18 FDG PET-CT for monitoring therapeutic effects of ipilimumab on melanoma lesions.
Introduction
It is estimated by the American Cancer Society that melanoma of the skin will affect 76,100 patients in the United States in 2014 and will cause approximately 9710 deaths. In the male population of the United States, melanoma will be the fifth leading newly diagnosed type of cancer after prostate, lung and bronchus, colon and rectum, and urinary bladder. The lifetime risk of developing melanoma of the skin for men is estimated to be 1 in 34 (American Cancer Society).
Metastatic melanoma is commonly treated with systemic chemotherapeutic agents including, but not limited to, interferon alpha (IFNα), pegylated IFN, vemurafenib, High dose interleukin-2 (HD-IL2), dacarbazine, temozolomide, platinum compounds, and taxanes. A meta-analysis conducted in 2010 by Tarhini and Thalanayar on IFNα treatment showed 18% and 11% risk reduction for recurrence and death, respectively . However, there are many side effects of IFNα, including fatigue, fever, weight loss, thyroid dysfunction, reversible hepatic dysfunction, myelosuppression, and depression . High-dose IL-2 has been used in a subset of patients with Eastern Cooperative Oncology Group (ECOG) of 0 and excellent organ function, with progression-free survival of 8.9 months and median survival of 12 months for responders. However, the side effects can be severe and can include hypotension, arrhythmia, fever, chills, metabolic acidosis, neurotoxicity, nausea, dyspnea, oliguria, and rash . As a result, overall survival in patients receiving IL-2 has not been evaluated in randomized phase III trials .
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Materials and Methods
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Table 1
Immune-mediated Side Effects Detected by F-18 fluorodeoxyglucose (F-18 FDG) PET-CT
Side Effect FDG PET Findings CT Findings Pancreatitis Diffusely elevated pancreatic FDG uptake Loss of normal pancreatic lobulation Colitis Elevated FDG uptake involving the ascending colon Fluid-filled ascending colon with mild pericolonic stranding Hypophysitis Focally elevated uptake in the pituitary gland No correlative findings on localization CT Thyroiditis Bilateral elevated thyroid gland uptake No nodularity or CT findings
PET-CT, positron emission tomography-computed tomography.
Get Radiology Tree app to read full this article<
Case 1
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Case 2
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Case 3
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Case 4
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Acknowledgment
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Tarhini A.A., Thalanayar P.M.: Melanoma adjuvant therapy. Hematol Oncol Clin North Am 2014; 28: pp. 471-489.
2. Palathinkal D.M., Sharma T.R., Koon H.B., et. al.: Current systemic therapies for melanoma. Dermatol Surg 2014; 40: pp. 948-963.
3. Garbe C., Eigentler T.K., Keilholz U., et. al.: Systematic review of medical treatment in melanoma: current status and future prospects. Oncologist 2011; 16: pp. 5-24.
4. Schadendorf D., Hodi F.S., Robert C., et. al.: Pooled analysis of long-term survival data from Phase II and Phase III trials of Ipilimumab in unresectable or metastatic melanoma. J Clin Oncol 2015; 33: pp. 1889-1894.
5. Agarwala S.S.: Current systemic therapy for metastatic melanoma. Expert Rev Anticancer Ther 2009; 9: pp. 587-595.
6. Joseph R.W., Eckel-Passow J.E., Sharma R., et. al.: Characterizing the clinical benefit of ipilimumab in patients who progressed on high-dose IL-2. J Immunother 2012; 35: pp. 711-715.
7. Hodi F.S., O’Day S.J., McDermott D.F., et. al.: Improved survival with ipilimumab in patients with metastatic melanoma. N Engl J Med 2010; 363: pp. 711-723.
8. Goethals L., Wilgenhof S., De Geeter F., et. al.: 18F-FDG PET/CT imaging of an anti-CTLA-4 antibody-associated autoimmune pancolitis. Eur J Nucl Med Mol Imaging 2011; 38: pp. 1390-1391.
9. BMS : YERVOY® (ipilimumab) injection, for intravenous infusion. Initial U.S. Approval. Bristol-Myers Squibb Company Princeton, NJ 08543 USA; Available at: http://packageinserts.bms.com/pi/pi_yervoy.pdf Accessed Oct 11, 2015.
10. Tarhini A.: Immune-mediated adverse events associated with ipilimumab CTLA-4 blockade therapy: the underlying mechanisms and clinical management. Scientifica (Cairo) 2013; 2013: pp. 857519.
11. Yousaf N., Davidson M., Goode E., et. al.: The cost of ipilimumab toxicity: a single-centre analysis. Melanoma Res 2015; 25: pp. 259-264.
12. Ryder M., Callahan M., Postow M.A., et. al.: Endocrine-related adverse events following ipilimumab in patients with advanced melanoma: a comprehensive retrospective review from a single institution. Endocr Relat Cancer 2014; 21: pp. 371-381.
13. Dilling P., Walczak J., Pikiel P., et. al.: Multiple colon perforation as a fatal complication during treatment of metastatic melanoma with ipilimumab—case report. Pol Przegl Chir 2014; 86: pp. 94-96.
14. Kim K.W., Ramaiya N.H., Krajewski K.M., et. al.: Ipilimumab-associated colitis: CT findings. AJR Am J Roentgenol 2013; 200: pp. W468-W474.
15. Lazaga F.J., Oz O.K., Adams-Huet B., et. al.: Comparison of whole-body versus limited whole-body 18F-FDG PET/CT scan in malignant cutaneous melanoma. Clin Nucl Med 2013; 38: pp. 882-884.
16. Iyamu I., Wachsmann J., Truelson J., et. al.: Detection of widespread metastasis in a case of aggressive carcinoma showing thymus like differentiation (CASTLE Disease) using 18F-FDG PET/CT. Clin Nucl Med 2015; 40: pp. 689-691.
17. Peng F., Rabkin G., Muzik O.: Use of 2-deoxy-2-[F-18]-fluoro-D-glucose positron emission tomography to monitor therapeutic response by rhabdomyosarcoma in children: report of a retrospective case study. Clin Nucl Med 2006; 31: pp. 394-397.
18. Chin B.B., Lyengar S., Sabundayo B.P., et. al.: Standardized uptake values in 2-Deoxy-2-[18F]Fluoro-D-Glucose with positron emission tomography. Clinical significance of iterative reconstruction and segmented attenuation compared with conventional filtered back projection and measured attenuation correction. Mol Imaging Biol 2002; 4: pp. 294-300.
19. Etchebehere E.C., Romanato J.S., Santos A.O., et. al.: Impact of [F-18] FDG-PET/CT in the restaging and management of patients with malignant melanoma. Nucl Med Commun 2010; 31: pp. 925-930.
20. Sachpekidis C., Larribere L., Pan L., et. al.: Predictive value of early 18F-FDG PET/CT studies for treatment response evaluation to ipilimumab in metastatic melanoma: preliminary results of an ongoing study. Eur J Nucl Med Mol Imaging 2015; 42: pp. 386-396.
21. Murphy G., Hussey D., Metser U.: Non-cutaneous melanoma: is there a role for (18)F-FDG PET-CT?. Br J Radiol 2014; 87: pp. 20140324.
22. van der Hiel B., Blank C.U., Haanen J.B., et. al.: Detection of early onset of hypophysitis by (18)F-FDG PET-CT in a patient with advanced stage melanoma treated with ipilimumab. Clin Nucl Med 2013; 38: pp. e182-e184.
23. Lyall A., Vargas H.A., Carvajal R.D., et. al.: Ipilimumab-induced colitis on FDG PET/CT. Clin Nucl Med 2012; 37: pp. 629-630.
24. Raad R.A., Pavlick A., Kannan R., et. al.: Ipilimumab-induced hepatitis on 18F-FDG PET/CT in a patient with malignant melanoma. Clin Nucl Med 2015; 40: pp. 258-259.
25. Bacanovic S., Burger I.A., Stolzmann P., et. al.: Ipilimumab-induced adrenalitis: a possible pitfall in 18F-FDG-PET/CT. Clin Nucl Med 2015; 40: pp. e518-e519.
26. Gilardi L., Colandrea M., Vassallo S., et. al.: Ipilimumab-induced immunomediated adverse events: possible pitfalls in (18)F-FDG PET/CT interpretation. Clin Nucl Med 2014; 39: pp. 472-474.
27. Chodakiewitz Y., Brown S., Boxerman J.L., et. al.: Ipilimumab treatment associated pituitary hypophysitis: clinical presentation and imaging diagnosis. Clin Neurol Neurosurg 2014; 125: pp. 125-130.