
Highlights
Advanced modeled iterative reconstruction causes substantial reductions of coronary artery calcium scores.
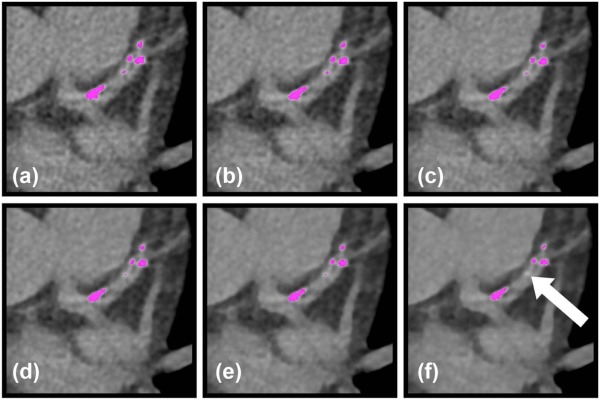
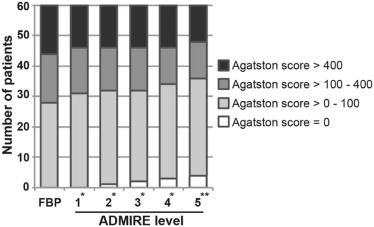
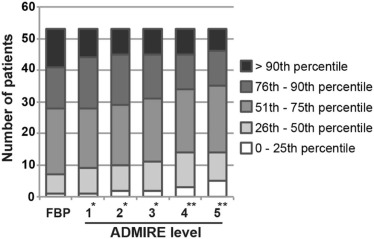
Coronary artery calcium may no longer be detectable using advanced modeled iterative reconstruction, especially in patients with low calcium burden.
Advanced modeled iterative reconstruction should be used with caution in coronary artery calcium scanning.
Rationale and Objectives
To evaluate the influence of advanced modeled iterative reconstruction (ADMIRE) on the coronary artery calcium (CAC) scores by computed tomography (CT).
Materials and Methods
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Conclusions
Get Radiology Tree app to read full this article<
Introduction
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Materials and Methods
Study Population
Get Radiology Tree app to read full this article<
Table 1
Patient Characteristics and CT Acquisition Parameters
Male/female 38 (63%)/22 (37%) Age (years) 63.1 ± 11.7 BMI (kg/m 2 ) 27.7 ± 5.9 Weight (kg) 81.3 ± 20.0 Height (m) 1.71 ± 0.1 Heart rate during scan (beats/min) 76 ± 18 CTDI VOL (mGy) 1.96 ± 0.93 DLP (mGy × cm) 31.9 ± 15.2 Scan length (cm) 11.9 ± 2.5 Effective dose (mSv) 0.45 ± 0.21
BMI, body mass index; CT, computed tomography; CTDI vol , the volume CT dose index; DLP, dose length product; presented as N (%) and mean ± SD.
Get Radiology Tree app to read full this article<
CAC Image Acquisition
Get Radiology Tree app to read full this article<
Image Reconstruction and Evaluation
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Results
Image Quality Parameters
Get Radiology Tree app to read full this article<
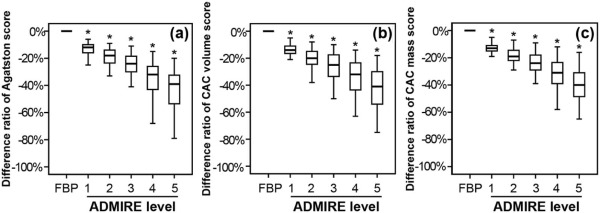
CAC Scoring
Get Radiology Tree app to read full this article<
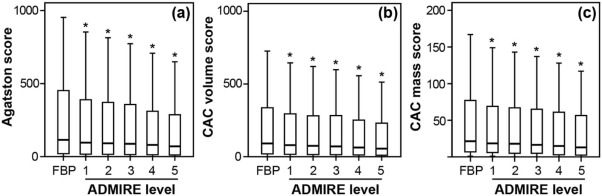
Table 2
Median Values and Difference Ratios of Coronary Agatston, Volumes, and Mass Scores for FBP and Incremental Strength Levels of ADMIRE
FBP ADMIRE 1 \* ADMIRE 2 \* ADMIRE 3 \* ADMIRE 4 \* ADMIRE 5 \* CAC Agatston Absolute 115 96 91 87 80 70 [23–450] [20–387] [19–367] [16–350] [14–310] [12–285] (0.1–3047) (0.1–2813) (0–2764) (0–2700) (0–2590) (0–2440) Difference ratio 0% −12% −18% −24% −32% −39% [−16–−10%] [−23–−14%] [−30–−18%] [−43–−26%] [−53–−33%] (−32–0%) (−100–−9%) (−100–−11%) (−100–−15%) (−100–−20%) CAC volume Absolute 91 79 74 70 63 55 [20–332] [17–293] [16–278] [14–281] [12–245] [10–224] (0–2468) (0–2273) (0–2226) (0–2172) (0–2070) (0–1956) Difference ratio 0% −14% −20% −25% −32% −41% [−16–−11%] [−25–−15%] [−34–−18%] [−44–−24%] [−54–−30%] (−50–0%) (−100–−8%) (−100–−10%) (−100–−14%) (−100–−18%) CAC mass Absolute 20 18 16 15 14 12 [4–77] [4–68] [3–66] [3–64] [3–59] [2–55] (0.03–618) (0.03–576) (0–567) (0–553) (0–531) (0–504) Difference ratio 0% −13% −19% −24% −31% −40% [−15–−11%] [−22–−15%] [−29–−18%] −39–−24%] [−49–−31%] (−31.4–0%) (−100–−7.2%) (−100–−9%) (−100–−12%) (−100–−16%)
ADMIRE, advanced modeled iterative reconstruction; CAC, coronary artery calcium; FBP, filtered back projection.
Data are presented as median [25th to 75th percentile] and (range). Difference ratio of different ADMIRE strength levels is calculated in comparison to FBP as reference.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Arad Y., Goodman K.J., Roth M., et. al.: Coronary calcification, coronary disease risk factors, C-reactive protein, and atherosclerotic cardiovascular disease events: the St. Francis Heart Study. J Am Coll Cardiol 2005; 46: pp. 158-165.
2. Lim S., Choi H.J., Shin H., et. al.: Subclinical atherosclerosis in a community-based elderly cohort: the Korean Longitudinal Study on Health and Aging. Int J Cardiol 2012; 155: pp. 126-133.
3. Sangiorgi G., Rumberger J.A., Severson A., et. al.: Arterial calcification and not lumen stenosis is highly correlated with atherosclerotic plaque burden in humans: a histologic study of 723 coronary artery segments using nondecalcifying methodology. J Am Coll Cardiol 1998; 31: pp. 126-133.
4. Detrano R., Guerci A.D., Carr J.J., et. al.: Coronary calcium as a predictor of coronary events in four racial or ethnic groups. N Engl J Med 2008; 358: pp. 1336-1345.
5. Taylor A.J., Bindeman J., Feuerstein I., et. al.: Coronary calcium independently predicts incident premature coronary heart disease over measured cardiovascular risk factors: mean three-year outcomes in the Prospective Army Coronary Calcium (PACC) project. J Am Coll Cardiol 2005; 46: pp. 807-814.
6. Greenland P., LaBree L., Azen S.P., et. al.: Coronary artery calcium score combined with Framingham score for risk prediction in asymptomatic individuals. JAMA 2004; 291: pp. 210-215.
7. Mollet N.R., Cademartiri F., van Mieghem C.A., et. al.: High-resolution spiral computed tomography coronary angiography in patients referred for diagnostic conventional coronary angiography. Circulation 2005; 112: pp. 2318-2323.
8. Achenbach S., Anders K., Kalender W.A.: Dual-source cardiac computed tomography: image quality and dose considerations. Eur Radiol 2008; 18: pp. 1188-1198.
9. Einstein A.J., Henzlova M.J., Rajagopalan S.: Estimating risk of cancer associated with radiation exposure from 64-slice computed tomography coronary angiography. JAMA 2007; 298: pp. 317-323.
10. Takx R.A., Schoepf U.J., Moscariello A., et. al.: angiography: comparison of a novel iterative reconstruction with filtered back projection for reconstruction of low-dose CT-Initial experience. Eur J Radiol 2013; 82: pp. 275-280.
11. Gordic S., Morsbach F., Schmidt B., et. al.: Ultralow-dose chest computed tomography for pulmonary nodule detection: first performance evaluation of single energy scanning with spectral shaping. Invest Radiol 2014; 49: pp. 465-473.
12. Gebhard C., Fiechter M., Fuchs T.A., et. al.: Coronary artery calcium scoring: influence of adaptive statistical iterative reconstruction using 64-MDCT. Int J Cardiol 2013; 167: pp. 2932-2937.
13. Kurata A., Dharampal A., Dedic A., et. al.: Impact of iterative reconstruction on CT coronary calcium quantification. Eur Radiol 2013; 23: pp. 3246-3252.
14. Takahashi M., Kimura F., Umezawa T., et. al.: Comparison of adaptive statistical iterative and filtered back projection reconstruction techniques in quantifying coronary calcium. J Cardiovasc Comput Tomogr 2016; 10: pp. 61-68.
15. McQuiston A.D., Muscogiuri G., Schoepf U.J., et. al.: Approaches to ultra-low radiation dose coronary artery calcium scoring based on 3rd generation dual-source CT: a phantom study. Eur J Radiol 2016; 85: pp. 39-47.
16. Christner J.A., Kofler J.M., McCollough C.H.: Estimating effective dose for CT using dose-length product compared with using organ doses: consequences of adopting International Commission on Radiological Protection publication 103 or dual-energy scanning. AJR Am J Roentgenol 2010; 194: pp. 881-889.
17. McClelland R.L., Chung H., Detrano R., et. al.: Distribution of coronary artery calcium by race, gender, and age: results from the Multi-Ethnic Study of Atherosclerosis (MESA). Circulation 2006; 113: pp. 30-37.
18. Budoff M.J., McClelland R.L., Chung H., et. al.: Reproducibility of coronary artery calcified plaque with cardiac 64-MDCT: the Multi-Ethnic Study of Atherosclerosis. AJR Am J Roentgenol 2009; 192: pp. 613-617.
19. Oudkerk M., Stillman A.E., Halliburton S.S., et. al.: Coronary artery calcium screening: current status and recommendations from the European Society of Cardiac Radiology and North American Society for Cardiovascular Imaging. Int J Cardiovasc Imaging 2008; 24: pp. 645-671.
20. Weininger M., Ritz K.S., Schoepf U.J., et. al.: Interplatform reproducibility of CT coronary calcium scoring software. Radiology 2012; 265: pp. 70-77.
21. Willemink M.J., Vliegenthart R., Takx R.A., et. al.: Coronary artery calcification scoring with state-of-the-art CT scanners from different vendors has substantial effect on risk classification. Radiology 2014; 273: pp. 695-702.
22. Schindler A., Vliegenthart R., Schoepf U.J., et. al.: Iterative image reconstruction techniques for CT coronary artery calcium quantification: comparison with traditional filtered back projection in vitro and in vivo. Radiology 2014; 270: pp. 387-393.
23. Murazaki H., Funama Y., Hatemura M., et. al.: Quantitative evaluation of calcium (content) in the coronary artery using hybrid iterative reconstruction (iDose) algorithm on low-dose 64-detector CT: comparison of iDose and filtered back projection. Nihon Hoshasen Gijutsu Gakkai Zasshi 2011; 67: pp. 360-366.
24. Gordic S., Desbiolles L., Sedlmair M., et. al.: Optimizing radiation dose by using advanced modelled iterative reconstruction in high-pitch coronary CT angiography. Eur Radiol 2016; 26: pp. 459-468.
25. Budoff M.J., Achenbach S., Blumenthal R.S., et. al.: Assessment of coronary artery disease by cardiac computed tomography: a scientific statement from the American Heart Association Committee on Cardiovascular Imaging and Intervention, Council on Cardiovascular Radiology and Intervention, and Committee on Cardiac Imaging, Council on Clinical Cardiology. Circulation 2006; 114: pp. 1761-1791.
26. Sarwar A., Shaw L.J., Shapiro M.D., et. al.: Diagnostic and prognostic value of absence of coronary artery calcification. JACC Cardiovasc Imaging 2009; 2: pp. 675-688.
27. Georgiou D., Budoff M.J., Kaufer E., et. al.: Screening patients with chest pain in the emergency department using electron beam tomography: a follow-up study. J Am Coll Cardiol 2001; 38: pp. 105-110.
28. Laudon D.A., Vukov L.F., Breen J.F., et. al.: Use of electron-beam computed tomography in the evaluation of chest pain patients in the emergency department. Ann Emerg Med 1999; 33: pp. 15-21.
29. McLaughlin V.V., Balogh T., Rich S.: Utility of electron beam computed tomography to stratify patients presenting to the emergency room with chest pain. Am J Cardiol 1999; 84: pp. 327-328. A8
30. Szilveszter B., Elzomor H., Karolyi M., et. al.: The effect of iterative model reconstruction on coronary artery calcium quantification. Int J Cardiovasc Imaging 2016; 32: pp. 153-160.