
Rationale and Objectives
Assess the impact of implementing a structured report template and a computer-aided diagnosis (CAD) tool on the quality of prostate multiparametric magnetic resonance imaging (mp-MRI) reports.
Materials and Methods
Institutional Review Board approval was obtained for this Health Insurance Portability and Accountability Act–compliant study performed at an academic medical center. The study cohort included all prostate mp-MRI reports ( n = 385) finalized 6 months before and after implementation of a structured report template and a CAD tool (collectively the information technology [IT] tools) integrated into the picture archiving and communication system workstation. Primary outcome measure was quality of prostate mp-MRI reports. An expert panel of our institution’s subspecialty-trained abdominal radiologists defined prostate mp-MRI report quality as optimal, satisfactory, or unsatisfactory based on documentation of nine variables. Reports were reviewed to extract the predefined quality variables and determine whether the IT tools were used to create each report. Chi-square and Student’s t tests were used to compare report quality before and after implementation of IT tools.
Results
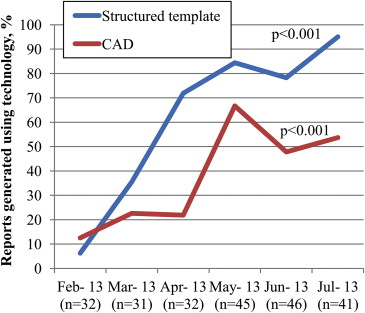
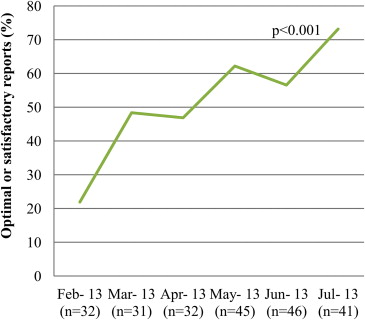
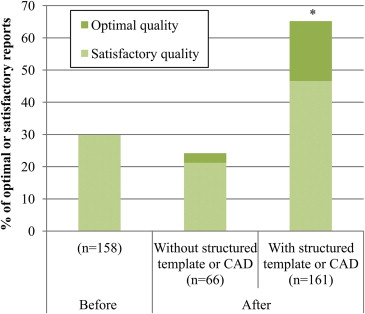
The overall proportion of optimal or satisfactory reports increased from 29.8% (47/158) to 53.3% (121/227) ( P < .001) after implementing the IT tools. Although the proportion of optimal or satisfactory reports increased among reports generated using at least one of the IT tools (47/158 = [29.8%] vs. 105/161 = [65.2%]; P < .001), there was no change in quality among reports generated without use of the IT tools (47/158 = [29.8%] vs. 16/66 = [24.2%]; P = .404).
Conclusions
The use of a structured template and CAD tool improved the quality of prostate mp-MRI reports compared to free-text report format and subjective measurement of contrast enhancement kinetic curve.
Multiparametric magnetic resonance imaging (mp-MRI) is a well-established, noninvasive modality for prostate cancer diagnosis , staging , biopsy targeting , and treatment planning . However, variation in what results are reported and how they are presented remains a barrier to widespread adoption of mp-MRI in clinical practice .
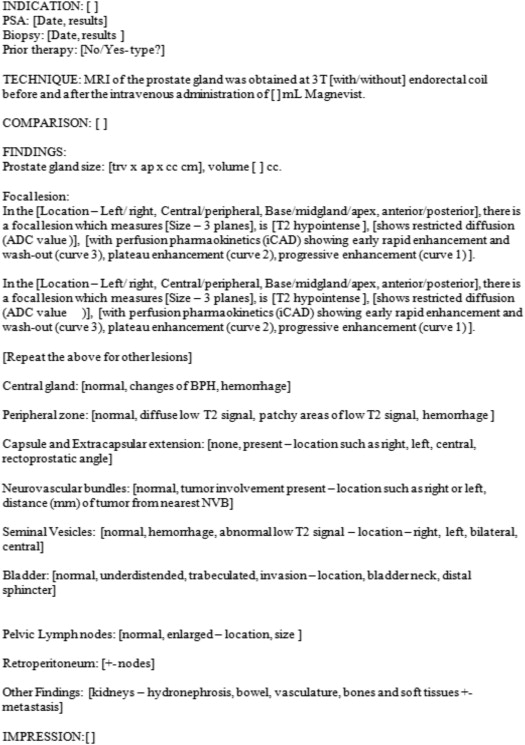
Measuring the quality of radiology reports is a complex task , particularly because of the lack of report standardization and objective key performance indicators . Free-text reports are typically not standardized, thus varying in content and format. Structured report templates have been developed to provide a consistent format and promote use of standard terminology . Compared to conventional, free-text reports, in addition to improving communication of test results, structured reports allow information to be retrieved and reused more easily . However, evidence of the impact of structured templates on the quality of radiology reports compared to free-text format is inconsistent .
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Materials and methods
Study Design and Setting
Get Radiology Tree app to read full this article<
Intervention
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Study Population
Get Radiology Tree app to read full this article<
Outcome Measures
Get Radiology Tree app to read full this article<
Table 1
Categorization of the Quality of Prostate Mp-MRI Reports
Quality Variables ∗ Report Quality Categories Optimal Satisfactory Unsatisfactory Prostate size Volume 3 Planes <3 Planes Focal lesion size 3 Planes or volume ≥2 Planes <2 Planes Restricted diffusion ADC value Documented Not documented Contrast enhancement Curve or quality † Documented Not documented T1 intensity/hemorrhage Documented Not documented Not documented T2 intensity Documented Documented Not documented Focal lesion segmental location ‡ Documented Documented Not documented Local invasion § Documented Documented Not documented Lymph nodes involvement Documented Documented Not documented
ADC, apparent diffusion coefficient; Mp-MRI, multiparametric magnetic resonance imaging.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Data Collection
Get Radiology Tree app to read full this article<
Statistical Analysis and Sample Size
Get Radiology Tree app to read full this article<
Results
Patient and Report Characteristics
Get Radiology Tree app to read full this article<
Table 2
Patient-Related Characteristics Based on 385 Prostate Multiparametric Magnetic Resonance Imaging Reports
Characteristic Before ( n = 158) After ( n = 227)P Value Age (mean [years] ± standard deviation [SD]) ∗ 64.2 ± 8.6 63.3 ± 9.1 0.293 Prostate-specific antigen (PSA) documented † 125/158 (79.1) 194/227 (85.5) 0.104 PSA (mean [ng/mL] ± SD) ∗ 8.1 ± 12.2 8.2 ± 7.4 0.880 Biopsy-proven cancer documented † 140/158 (88.6) 187/227 (82.4) 0.093 Gleason documented † 105/158 (66.5) 159/227 (70.0) 0.456 Gleason (mean ± SD) ∗ 6.88 ± 0.9 6.83 ± 1.0 0.668 Focal lesion present † 121/152 (79.6) 170/224 (75.9) 0.398
Data presented in the parenthesis are percentages.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Structured Template and CAD Tool Utilization
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Report Quality
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 3
Documentation of Quality Variables Before and After the Implementation of a Structured Report Template and a Computer-Aided Diagnosis Tool
Quality Variables ∗ Before ( n = 158) After ( n = 227)P Value Prostate size in three planes 151 (95.6) 205 (90.3) 0.054 Prostate volume 149 (94.3) 222 (97.8) 0.072 Focal lesion presence documented 152 (96.2) 224 (98.7) 0.114 Focal lesion segmental location † 117 (74.1) 166 (73.1) 0.840 Focal lesion size ‡ ≥2 Planes 79 (65.3) 137 (80.6)0.003 Three planes or volume 24 (19.8) 73 (42.9)<0.001 Restricted diffusion Documented 139 (88.0) 202 (89.0) 0.759 ADC value 1 (0.63) 100 (44.1)<0.001 Contrast enhancement Documented 111 (70.3) 183 (80.6)0.019 Curve/quality § 4 (2.5) 87 (38.3)<0.001 T2 intensity 152 (96.2) 214 (94.3) 0.390 T1 intensity 78 (49.4) 115 (50.7) 0.803 Local invasion ‖ 131 (82.9) 213 (93.8)<0.001 Lymph nodes involvement 156 (100) 155 (99.6) 0.404
Data presented in the parenthesis are percentages. Values in bold are statistically significant.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Conclusions
Get Radiology Tree app to read full this article<
Supplementary Data
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Turkbey B., Pinto P.A., Mani H., et. al.: Prostate cancer: value of multiparametric MR imaging at 3 T for detection–histopathologic correlation. Radiology 2010; 255: pp. 89-99.
2. Nix J.W., Turkbey B., Hoang A., et. al.: Very distal apical prostate tumours: identification on multiparametric MRI at 3 Tesla. BJU Int 2012; 110: pp. E694-E700.
3. Fütterer J.J., Engelbrecht M.R., Huisman H.J., et. al.: Staging prostate cancer with dynamic contrast-enhanced endorectal MR imaging prior to radical prostatectomy: experienced versus less experienced readers. Radiology 2005; 237: pp. 541-549.
4. Hegde J.V., Chen M.-H., Mulkern R.V., et. al.: Preoperative 3-Tesla multiparametric endorectal magnetic resonance imaging findings and the odds of upgrading and upstaging at radical prostatectomy in men with clinically localized prostate cancer. Int J Radiat Oncol Biol Phys 2013; 85: pp. e101-e107.
5. Franiel T., Stephan C., Erbersdobler A., et. al.: Areas suspicious for prostate cancer: MR-guided biopsy in patients with at least one transrectal US-guided biopsy with a negative finding—multiparametric MR imaging for detection and biopsy planning. Radiology 2011; 259: pp. 162-172.
6. Sciarra A., Panebianco V., Cattarino S., et. al.: Multiparametric magnetic resonance imaging of the prostate can improve the predictive value of the urinary prostate cancer antigen 3 test in patients with elevated prostate-specific antigen levels and a previous negative biopsy. BJU Int 2012; 110: pp. 1661-1665.
7. Turkbey B., Mani H., Aras O., et. al.: Prostate cancer: can multiparametric MR imaging help identify patients who are candidates for active surveillance?. Radiology 2013; 268: pp. 144-152. Available at: http://radiology.rsna.org/content/early/2013/02/28/radiol.13121325
8. Gupta R.T., Kauffman C.R., Polascik T.J., et. al.: The state of prostate MRI in 2013. Oncology (Williston Park) 2013; 27: pp. 262-270.
9. Dickinson L., Ahmed H.U., Allen C., et. al.: Clinical applications of multiparametric MRI within the prostate cancer diagnostic pathway. Urol Oncol 2013; 31: pp. 281-284.
10. Pool F., Goergen S.: Quality of the written radiology report: a review of the literature. J Am Coll Radiol 2010; 7: pp. 634-643.
11. Reiner B.: Uncovering and improving upon the inherent deficiencies of radiology reporting through data mining. J Digit Imaging 2010; 23: pp. 109-118.
12. Prevedello L.M., Farkas C., Ip I.K., et. al.: Large-scale automated assessment of radiologist adherence to the Physician Quality Reporting System for stroke. J Am Coll Radiol 2012; 9: pp. 414-420.
13. Weiss D.L., Langlotz C.P.: Structured reporting: patient care enhancement or productivity nightmare?. Radiology 2008; 249: pp. 739-747.
14. Johnson A.J., Chen M.Y.M., Swan J.S., et. al.: Cohort study of structured reporting compared with conventional dictation. Radiology 2009; 253: pp. 74-80.
15. Dickinson L., Ahmed H.U., Allen C., et. al.: Magnetic resonance imaging for the detection, localisation, and characterisation of prostate cancer: recommendations from a European Consensus Meeting. Eur Urol 2011; 59: pp. 477-494.
16. Barentsz J.O., Richenberg J., Clements R., et. al.: ESUR prostate MR guidelines 2012. Eur Radiol 2012; 22: pp. 746-757.
17. International Scientific Cooperation to Advance Image Guided Prostate Cancer Care—American College of Radiology, AdMeTech Foundation and European Society of Urogenital Radiology create standards for high quality MRI. [cited 2014 May 22]. Available at: http://www.acr.org/About-Us/Media-Center/Press-Releases/2012-Press-Releases/20120207-International-Scientific-Cooperation-to-Advance-Image-Guided-Prostate-Cancer-Care . Accessed May 22, 2014.
18. Dorrius M.D., Jansen-van der Weide M.C., van Ooijen P.M.A., et. al.: Computer-aided detection in breast MRI: a systematic review and meta-analysis. Eur Radiol 2011; 21: pp. 1600-1608.
19. Giger M.L., Chan H.-P., Boone J.: Anniversary paper: history and status of CAD and quantitative image analysis: the role of Medical Physics and AAPM. Med Phys 2008; 35: pp. 5799-5820.
20. Peng Y., Jiang Y., Yang C., et. al.: Quantitative analysis of multiparametric prostate MR images: differentiation between prostate cancer and normal tissue and correlation with Gleason Score—a Computer-Aided Diagnosis Development Study. Radiology 2013; 267: pp. 787-796.
21. Hoeks C.M.A., Barentsz J.O., Hambrock T., et. al.: Prostate cancer: multiparametric MR imaging for detection, localization, and staging. Radiology 2011; 261: pp. 46-66.
22. Allen B., Levin D.C., Brant-Zawadzki M., et. al.: ACR white paper: strategies for radiologists in the era of health care reform and accountable care organizations: a report from the ACR Future Trends Committee. J Am Coll Radiol 2011; 8: pp. 309-317.
23. Quentin M., Blondin D., Klasen J., et. al.: Evaluation of a structured report of functional prostate magnetic resonance imaging in patients with suspicion for prostate cancer or under active surveillance. Urol Int 2012; 89: pp. 25-29.
24. Khorasani R., Bates D.W., Teeger S., et. al.: Is terminology used effectively to convey diagnostic certainty in radiology reports?. Acad Radiol 2003; 10: pp. 685-688.
25. Plumb A.A.O., Grieve F.M., Khan S.H.: Survey of hospital clinicians’ preferences regarding the format of radiology reports. Clin Radiol 2009; 64: pp. 386-394. 395–396
26. Kahn C.E., Heilbrun M.E., Applegate K.E.: From guidelines to practice: how reporting templates promote the use of radiology practice guidelines. J Am Coll Radiol 2013; 10: pp. 268-273.
27. Schwartz L.H., Panicek D.M., Berk A.R., et. al.: Improving communication of diagnostic radiology findings through structured reporting. Radiology 2011; 260: pp. 174-181.
28. Hambrock T., Vos P.C., Hulsbergen-van de Kaa C.A., et. al.: Prostate cancer: computer-aided diagnosis with multiparametric 3-T MR imaging—effect on observer performance. Radiology 2013; 266: pp. 521-530.
29. Raja A.S., Ip I.K., Prevedello L.M., et. al.: Effect of computerized clinical decision support on the use and yield of CT pulmonary angiography in the emergency department. Radiology 2012; 262: pp. 468-474.
30. Kash B.A., Spaulding A., Johnson C.E., et. al.: Success factors for strategic change initiatives: a qualitative study of healthcare administrators’ perspectives. J Healthc Manag 2014; 59: pp. 65-81.
31. Prevedello L.M., Farkas C., Dufault A., et. al.: Using informatics-enabled quality improvement techniques to meet health record documentation requirements in radiology reports. Acad Radiol 2013; 20: pp. 1032-1036.