
Rationale and Objectives
To increase detection of mislabeled medical imaging studies, evidence shows it may be useful to include patient photographs during interpretation. This study examined how inclusion of photographs impacts visual search.
Materials and Methods
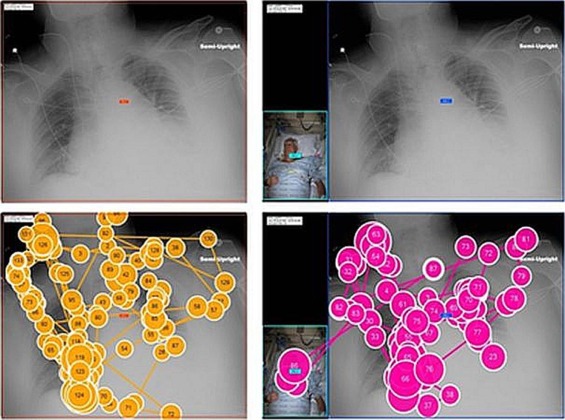
Ten radiologists participated. Average age was 43.00 years and average years Board-certified was 9.70, with 2 residents, 1 general, 2 abdominal, 4 cardiothoracic, and 1 pediatric radiologist. They viewed 21 portable chest radiographs with and without a simultaneously acquired photograph of the patient while visual search was recorded. Their task was to note placement of lines and tubes.
Results
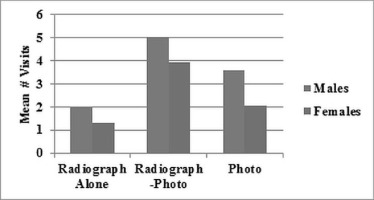
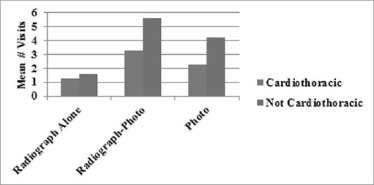
Presence of the photograph reduced the number of fixations (chest radiograph only mean 98.68; chest with photograph present 80.81; photograph 10.59; p < 0.0001) and total dwell (chest radiograph only mean 30.84 seconds; chest radiograph with photograph present 25.68; photograph 3.93; p < 0.0001) on the chest radiograph as a result of periodically looking at the photograph. Overall viewing time did not increase with addition of the photograph because time not spent on the radiograph was spent on the photograph. On average, readers scanned from the radiograph to the photographs about four times during search. Men and non-cardiothoracic radiologists spent significantly more time scanning all the images, including the photographs. Average preference for having photographs was 6.10 on a 0–10 scale, and neck and chest were preferred as areas to include in the photograph.
Conclusion
Photographs may help with certain image interpretation tasks and may help personalize the reading experience for radiologists without increasing interpretation time.
Introduction
The Institute of Medicine’s Committee on Quality of Health Care in America estimated that as many as 98,000 people die each year from medical errors . In radiology, a potential source of error is the wrong-patient error , which happens when a patient’s radiograph is incorrectly filed under a different patient’s folder in the Picture Archiving and Communication System (PACS). For example, one Pennsylvania study demonstrated that 196 of 652 (30.1%) error events in radiology in 1 year that resulted in serious patient harm were wrong-patient errors .
To minimize such identification errors, The Joint Commission in its National Patient Safety Goals outlines the requirement of including at least two patient identifiers when providing care, treatment, and services. These identifiers may include the individual’s name, an assigned medical record number, telephone number, or other person-specific identifier, such as date of birth or social security number . However, when mobile or portable radiographs are obtained in high-stress environments outside of the radiology department, such as in the emergency department or in the intensive care unit (ICU), where patients often cannot accurately provide identification information due to sedation, intoxication, alteration in consciousness, or inability to communicate for other reasons, the setting is ripe for wrong-patient errors to occur .
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Material and Methods
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Radiologists
Get Radiology Tree app to read full this article<
Radiograph Review Task Design
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Eye-Tracking Analysis
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Survey and Data Analysis
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Table 1
Radiologists’ Frequency of Responses in Each Category for the Pre- and Post-Study Surveys with Test Value and P -Value in the Right Columns
Question Significantly Less Slightly Less No Difference Slightly More Significantly More χ 2 P -Value Pre-study (without photos) Call referring critical result 0 0 0 0 10 40.00 <.0001 Call referring important finding 0 0 1 2 7 17.00 <.001 Look up patient info 0 0 1 0 9 31.00 <.0001 Post-study (with photos) Accurate interpretation images 0 1 2 5 2 7.00 NS Accurate interpretation lines and tubes 0 1 0 4 5 11.00 <.05 Accurate ID mislabeled patients 0 0 1 7 2 17.00 <.001 Accurate evaluation health status 0 0 3 5 2 9.00 NS Spend time interpretation 0 1 2 5 2 7.00 NS Comfortable photo present 0 3 4 2 1 5.00 NS Distracted photo present 1 0 6 2 1 11.00 <.05 Call referring critical with photo 0 0 7 2 1 17.00 <.001 Call referring important with photo 0 0 6 3 1 13.00 <.02 Look up patient info with photo 0 2 6 1 1 11.00 <.05
NS, not significant.
Table 2
Radiologists’ Frequency of Yes Versus No Responses for Which Body Areas Should Be Included in the Photographs with Test Value and P -Value in the Right Columns
Areas to Include Yes No χ 2 P -Value Face 5 5 0.00 NS Neck 9 1 6.40 .02 Chest 8 2 3.60 NS Abdomen 3 7 1.60 NS
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 3
Results of the Eye-Tracking Study Using ANOVA with the Means and Standard Deviations for Each of the Three Images
Eye-Tracking Parameter Radiograph Alone (1)
(SD) Radiograph with Photograph (2) Photograph (3) F-Value_P_ -Value PLSD No. of fixations 98.68(68.43) 80.81(53.99) 10.59(9.59) 198.93 <.0001 1 vs 3 1 vs 3 2 vs 3 Mean fixation duration (s) 0.31(0.04) 0.30(0.04) 0.37(0.14) 40.19 <.0001 1 vs 3 2 vs 3 Total dwell (s) 30.84(21.07) 25.68(28.24) 3.93(3.81) 90.82 <.0001 1 vs 2 1 vs 3 2 vs 3 Dwell first fixation (s) 0.23(0.13) 0.22(0.13) 0.30(0.19) 11.69 <.0001 1 vs 3 2 vs 3 No. of visits to image 1.77(2.16) 4.70(3.31) 3.15(2.85) 104.70 <.0001 1 vs 2 1 vs 3 2 vs 3
ANOVA, analysis of variance; PLSD, protected least squares difference; SD, standard deviation.
Note: The last column on the right shows which conditions differed significantly when tested with the PLSD test (1 = radiograph alone, 2 = radiograph with photograph, 3 = photograph).
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Prior Work
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Limitations
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Conclusions
Get Radiology Tree app to read full this article<
Acknowledgements
Get Radiology Tree app to read full this article<
Appendix
Get Radiology Tree app to read full this article<
Please mark the best option: Significantly less Slightly less No difference Slightly more Significantly more I am______ likely to call the referring provider if I detect a critical result. I am______ likely to call the referring provider if I detect an important finding. I am______ likely to look up patient information in the electronic medical record to clarify my report if I am unsure of the radiographic findings. Your age: Your gender (circle one):
Male/Female Subspecialty area of practice:
(a) In training
(b) General Radiologist
(c) Body
(d ) Breast
(e) Cardiothoracic
(f) Interventional
(g) Musculoskeletal
(h) Neuroradiology
(i) Pediatric Years in practice as a Board-certified radiologist: ___years
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Please mark the best option: Significantly less Slightly less No difference Slightly more Significantly more Having patients’ photographs available: could result in ______accurate interpretation of images. could result in ______accurate interpretation of lines and tubes. could result in ______accurate identification of mislabeled patients. could result in ______accurate evaluation of patient health status. could result in spending ______ time for interpretation of imaging test. I felt ______ comfortable interpreting imaging tests with the photographs present. I felt ______ distracted from concentrating on accurate imaging interpretation with the photographs present. I would be______ likely to call a report to the referring provider if I detect a critical result with the photographs present than without. I would be______ likely to call the referring provider if I detect an important finding with the photographs present than without. I would be______ likely to look up patient information in the electronic medical record to clarify my report if I am unsure of the radiographic findings with the photographs present than without.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
 Open full size image
Open full size image
Your age: Your gender (circle one):
Male/Female In your opinion, which body parts should be included in the patient’s photograph for a chest radiograph? (Check all that apply.)
(a) Face
(b) Neck
(c) Chest
(d) Abdomen
(e) Other (please specify ) _____________ Subspecialty area of practice:
(j) In training
(k) General Radiologist
(l) Body
(m) Breast
(n) Cardiothoracic
(o) Interventional
(p) Musculoskeletal
(q) Neuroradiology
(r) Pediatric Years in practice as a Board-certified radiologist: ___years
Get Radiology Tree app to read full this article<
References
1. Committee on Quality of Health Care in America, Institute of Medicine : Kohn L.T.Corrigan J.M.Donaldson M.S.To err is human: building a safer health system.2000.National Academy of SciencesWashington, DC:
2. Pennsylvania Patient Safety Advisory : Applying the universal protocol to improve patient safety in radiology. PA Pat Saf Auth 2011; 8: pp. 63-70. Available at http://patientsafetyauthority.org/ADVISORIES/AdvisoryLibrary/2011/jun8%282%29/Pages/63.aspx Accessed January 28, 2016
3. Joint Commission on Accreditation of Healthcare Organizations : National patient safety goals. Available at: http://www.jointcommission.org/assets/1/6/2015_NPSG_HAP.pdf Accessed January 5, 2015
4. Park K.: Human error.Salvendy G.Handbook of human factors and ergonomics.1997.John Wiley & Son, IncNew York:pp. 163.
5. Ramamurthy S., Bhatti P., Arepalli C.D., et. al.: Integrating patient digital photographs with medical imaging examinations. J Digit Imaging 2013; 26: pp. 875-885.
6. Tridandapani S., Ramamurthy S., Galgano S.J., et. al.: Increasing rate of detection of wrong-patient radiographs: use of photographs obtained at time of radiography. AJR Am J Roentgenol 2013; 200: pp. W345-W352.
7. Tridandapani S., Ramamurthy S., Provenzale J., et. al.: A multiobserver study of the effects of including point-of-care patient photographs with portable radiography: a means to detect wrong-patient errors. Acad Radiol 2014; 21: pp. 1038-1047.
8. Sadigh G., Applegate K.E., Ng T.W., et. al.: Stakeholders’ perceptions regarding the use of patient photographs integrated with medical imaging studies. J Digit Imaging 2015; ePub ahead of print
9. Slasky B.S., Gur D., Good W.F., et. al.: Receiver operating characteristic analysis of chest image interpretation with conventional, laser-printed, and high-resolution workstation images. Radiology 1990; 174: pp. 775-780.
10. Duchowski A.: Eye tracking methodology: theory and practice.2007.Springer-VerlagLondon, England
11. Kundel H.L., Nodine C.F., Krupinski E.A., et. al.: Using gaze-tracking data and mixture distribution analysis to support a holistic model for the detection of cancers on mammograms. Acad Radiol 2008; 15: pp. 881-886.
12. Tourassi G.D., Mazurowski M.A., Harrawood B.P., et. al.: Exploring the potential of context-sensitive CADe in screening mammography. Med Phys 2010; 37: pp. 5728-5736.
13. Kundel H.L., Nodine C.F., Krupinski E.A.: Searching for lung nodules: visual dwell indicates locations of false-positive and false-negative decisions. Invest Radiol 1989; 24: pp. 472-478.
14. Krupinski E.A., Nodine C.F., Kundel H.L.: A perceptually-based method for enhancing pulmonary nodule recognition. Invest Radiol 1993; 28: pp. 289-294.
15. Helbren E., Halligan S., Phillips P., et. al.: Towards a framework for analysis of eye-tracking studies in the three dimensional environment: a study of visual search by experienced readers of endoluminal CT colonography. Br J Radiol 2014; 87: pp. 20130614.
16. AlMousa D.S., Brennan P.C., Ryan E.A., et. al.: How mammographic breast density affects radiologists’ visual search patterns. Acad Radiol 2014; 21: pp. 1386-1393.
17. Giovinco N.A., Sutton S.M., Miller J.D., et. al.: A passing glance? Differences in eye tracking and gaze patterns between trainees and experts reading plain film bunion radiographs. J Foot Ankle Surg 2015; 54: pp. 382-391.
18. Krupinski E.A., Chao J., Hofmann-Wellenhof R., et. al.: Understanding visual search patterns of dermatologists assessing pigmented skin lesions before and after online training. J Digit Imaging 2014; 27: pp. 779-785.
19. Krupinski E.A., Graham A.R., Weinstein R.S.: Characterizing the development of visual search expertise in pathology residents viewing whole slide images. Hum Pathol 2013; 44: pp. 357-364.
20. Nodine C.F., Kundel H.L., Toto L.C., et. al.: Recording and analyzing eye-position data using a microcomputer workstation. Behav Res Methods Instrum Comput 1992; 24: pp. 475-485.
21. Philpotts L.E.: Can computer-aided detection be detrimental to mammographic interpretation?. Radiology 2009; 253: pp. 17-22.
22. Tchou P.M., Haygood T.M., Atkinson E.N., et. al.: Interpretation time of computer-aided detection at screening mammography. Radiology 2010; 257: pp. 40-46.
23. Sadigh G., Loehfelm T., Applegate K.E., et. al.: Evaluation of near-miss wrong-patient events in radiology. AJR Am J Roentgenol 2015; 205: pp. 44-48.
24. Turner Y., Hadas-Halpern I.: The effects of including a patient’s photograph to the radiographic examination. Presented at; Radiological Society of North America Scientific Assembly and Annual Meeting; Oak Brook, Illinois2008.
25. Ryan J., Khanda G.E., Hibbert R., et. al.: Is a picture worth a thousand words? The effect of viewing patient photographs on radiologist interpretation of CT studies. J Am Coll Radiol 2015; pp. 104-107.