
Introduction
Lateral epicondylitis, commonly known as tennis elbow, is the most common cause of lateral elbow pain and the second most frequently diagnosed musculoskeletal disorder in the neck and upper limb in a primary care setting. Many therapeutic options, including conservative, surgical, and minimally invasive procedures, have been advocated for the treatment of lateral epicondylitis. Although numerous small studies have been performed to assess the efficacy of various treatments, there are conflicting results with no clear consensus on the optimal treatment. In an economic environment with limited health care resources, it is paramount that optimal cost-effective therapies with favorable patient-important outcomes be identified.
Methods and Analysis
This is a protocol paper which outlines a multicenter, multidisciplinary, single-blinded, four-arm randomized controlled trial, comparing platelet-rich plasma (PRP), whole blood injection, dry needle tendon fenestration, and sham injection with physical therapy alone for the treatment of lateral epicondylitis. Patients are screened based on pre-established eligibility criteria and randomized to one of the four study groups using an Internet-based system. The patients are followed at 6-week, 12-week, 24-week, and 52-week time points to assess the primary and secondary outcomes of the study. The primary outcome is pain. Secondary outcomes include health-related quality of life and ultrasound appearance of the common extensor tendon. Two university centers (McMaster University and the University of Michigan) are currently recruiting patients. We have planned a sample size of 100 patients (25 patients per arm) to ensure over 80% power to detect a three-point difference in pain scores at 52 weeks of follow-up.
Ethics and Dissemination
This study has ethics approval from the McMaster University Research Ethics Board (REB# 12-146) and the University of Michigan Institutional Review Board (IRB# HUM00067750). Successful completion of this proposed study will significantly impact clinical practice and enhance patients’ lives. More broadly, this trial will develop a network of collaboration from which further high-quality trials in ultrasound-guided interventions will follow.
Article Summary
Article Focus
Impact of platelet-rich plasma (PRP) over alternative therapies in patients with lateral epicondylitis (IMPROVE) is a multicenter, multidisciplinary, single-blinded, randomized controlled trial (RCT) comparing autologous PRP, autologous whole blood, dry needle tendon fenestration, and sham injection with physical therapy on pain and quality of life in patients with lateral epicondylitis.
Key Messages
Strengths and Limitations
- Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Magnitude of the Problem
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Lateral Epicondylitis (“Tennis Elbow”) Treatment Options
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
The Promise of PRP
Biologic Rationale for Use
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
PRP: Emerging Evidence, Lack of Definitive Results
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Need for Definitive Evidence
Get Radiology Tree app to read full this article<
Summary: Rationale for a Definitive RCT
Get Radiology Tree app to read full this article<
Materials and Methods
Study Design
Overview of Study Design
Get Radiology Tree app to read full this article<

Table 1
Summary of Study Design for the IMPROVE Study

PRP, platelet-rich plasma; PT, physical therapy.
Get Radiology Tree app to read full this article<
The Principal Research Questions
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Eligibility Criteria
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Recruitment and Screening
Get Radiology Tree app to read full this article<
Allocation of Patients to Study Groups
Get Radiology Tree app to read full this article<
Sonographic Assessment
Get Radiology Tree app to read full this article<
Table 2
Diagnostic Ultrasound Features for the IMPROVE Study
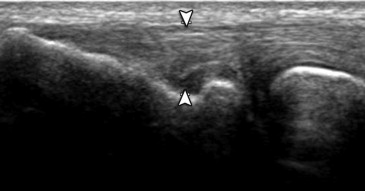
Diagnostic Feature Description Measurement Tendon echogenicity The degree of tendinosis is graded based on changes in tendon echotexture Grade 0: normal (excluded)
Grade 1: (mild) ill-defined abnormal hypoechogenicity
Grade 2: (moderate) well-defined abnormal echogenicity
Grade 3: (severe) well-defined abnormal hypoechogenicity and anechoic clefts
Grade 4: (complete) full-width disruption or tear (excluded)
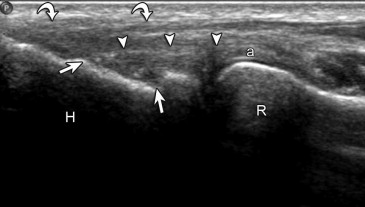
( Fig 3 ) Gray scale abnormality dimensions The greatest dimensions of the gray scale abnormality are measured in millimeters using this axis (1) Short axis
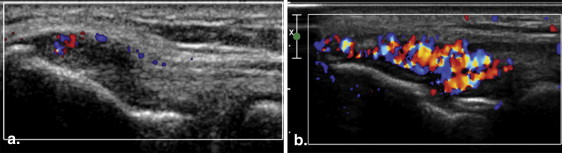
(2) Long axis Tendon thickness The maximal tendon thickness is measured in millimeters at the base of the lateral epicondyle, perpendicular to tendon, with transducer long axis to tendon ( Fig 4 ) Radial collateral ligament (RCL) The gray scale abnormality is described as involving the RCL or not involving the RCL ( Fig 5 ) Tendon hyperemia (involving gray scale abnormality long axis to tendon) The degree of blood flow to the tendon is measured by both color and power Doppler ultrasound None
Mild: a few pixels
Moderate: <50% of the tendon
Severe: >50% of the tendon
( Fig 6 ) Cortical irregularity of common extensor tendon The common extensor tendon footprint is described as having cortical irregularity or not having cortical irregularity Intratendinous calcification The intratendinous calcification is measured in millimeters at the largest dimension and graded None
Hyperechoic with shadowing
Hyperechoic without shadowing Enthesophyte The presence or lack of enthesophyte(s) is recorded
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<

Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Study Interventions
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Group A: PRP injection (+ physical therapy)
Get Radiology Tree app to read full this article<
Group B: whole blood injection (+ physical therapy)
Get Radiology Tree app to read full this article<
Group C: dry needle tendon fenestration (+ physical therapy)
Get Radiology Tree app to read full this article<
Group D: sham injection and physical therapy alone
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Bilateral Lateral Epicondylitis
Get Radiology Tree app to read full this article<
Blinding
Get Radiology Tree app to read full this article<
Threshold Performance for Expertise in Performing Autologous Blood Injections
Get Radiology Tree app to read full this article<
Periprocedural Treatment
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Outcome Measures
Get Radiology Tree app to read full this article<
Patient Follow-up
Get Radiology Tree app to read full this article<
Maximization of Follow-up
Get Radiology Tree app to read full this article<
Crossovers, Contamination, and Cointerventions
Get Radiology Tree app to read full this article<
Sample Size Consideration
Get Radiology Tree app to read full this article<
Data Analysis Plan
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Data Safety Monitoring Board
Get Radiology Tree app to read full this article<
Potential Impact of Study
Get Radiology Tree app to read full this article<
Acknowledgments
Get Radiology Tree app to read full this article<
References
1. Faro F., Wolf J.M.: Lateral epicondylitis: review and current concepts. J Hand Surg 2007; 32A: pp. 1271-1279.
2. Alizadehkhaiyat O., Fisher A.C., Kemp G.J., et. al.: Pain, functional disability, and psychologic status in tennis elbow. Clin J Pain 2007; 23: pp. 482-489.
3. Walker-Bone K., Palmer K.T., Reading I., et. al.: Occupation and epicondylitis: a population-based study. Rheumatology 2012; 51: pp. 305-310.
4. Nirschl R., Pettrone F.: Tennis elbow: the surgical treatment of lateral epicondylitis. JBJS 1979; 61A: pp. 832-841.
5. Connell D., Burke F., Coombes P., et. al.: Sonographic examination of lateral epicondylitis. AJR Am J Roentgenol 2001; 176: pp. 777-782.
6. Walz D.M., Newman J.S., Konin G.P., et. al.: Epicondylitis: pathogenesis, imaging, and treatment. Radiographics 2010; 30: pp. 167-184.
7. Nirschl R.P., Ashman E.S.: Elbow tendinopathy: tennis elbow. Clin Sports Med 2003; 22: pp. 813-836.
8. Kijowski R., Tuite M., Sanford M.: Magnetic resonance imaging of the elbow. Part II: abnormalities of the ligaments, tendons, and nerves. Skeletal Radiol 2005; 34: pp. 1-18.
9. Sheth U., Simunovic N., Guy Klein G.: The efficacy of autologous platelet rich plasma use in orthopaedic indications: a meta-analysis. J Bone Joint Surg Am 2012; 94: pp. 298-307.
10. Taylor D.W., Petrera M., Hendry M., et. al.: A systematic review of the use of platelet-rich plasma in sports medicine as a new treatment for tendon and ligament Injuries. Clin J Sport Med 2011; 21: pp. 344-352.
11. Binder A.I., Hazleman B.L.: Lateral humeral epicondylitis—a study of natural history and the effect of conservative therapy. Br J Rheumatol 1983; 22: pp. 73-76.
12. Price , Sinclair H., Heinrich I., et. al.: Local injection treatment of tennis elbow—hydrocortisone, triamcinolone and lignocaine compared. Br J Rheumatol 1991; 30: pp. 39-44.
13. Solveborn S.A., Buch F., Mallmin H., et. al.: Cortisone injection with anesthetic additives for radial epicondylalgia (tennis elbow). Clin Orthop Relat Res 1995; pp. 99-105.
14. Hay E.M., Paterson S.M., Lewis M., et. al.: Croft, Pragmatic randomised controlled trial of local corticosteroid injection and naproxen for treatment of lateral epicondylitis of elbow in primary care. BMJ 1999; 319: pp. 964-968.
15. Smidt N., van de Windt D.A., Assendelft W.J., et. al.: Corticosteroid injections, physiotherapy, or wait-and-see policy for lateral epicondylitis: a randomized controlled trial. Lancet 2002; 359: pp. 657-662.
16. Best T., Zgierska A.E., Zeisig E., et. al.: A systematic review of four injection therapies for lateral epicondylosis: prolotherapy, polidocanol, whole blood and platelet rich plasma. Br J Sports Med 2009; 43: pp. 471-481.
17. Korthals-de Bos I.B.C., Smidt N., van Tulde M.W.: Cost effectiveness of interventions for lateral epicondylitis results from a randomised controlled trial in primary care. Pharmacoeconomics 2004; 22: pp. 185-195.
18. Sampson S., Gerhardt M., Mandelbaum B.: Platelet rich plasma injection grafts for musculoskeletal injuries: a review. Curr Rev Musculoskelet Med 2008; 1: pp. 165-174.
19. Woodell-May J.E., Pietrzak W.S.: Platelet-rich plasma in orthopaedics.Pietrzak W.S.Vacanti C.A.Musculoskeletal tissue regeneration: biological materials and methods.2008.Springer-VerlagNew York, NY:pp. 547-568.
20. Anitua E., Andia I., Ardanza B., et. al.: Autologous platelets as a source of proteins for healing and tissue regeneration. Thromb Haemost 2004; 91: pp. 4-15.
21. Lopez-Vidriero L., Goulding K.A., Simon D.A., et. al.: The use of platelet-rich plasma in arthroscopy and sports medicine: optimizing the healing environment. Arthroscopy 2010; 26: pp. 269-278.
22. Edwards S.G., Calandruccio J.H.: Autologous blood injections for refractory lateral epicondylitis. J Hand Surg Am 2003; 28: pp. 272-278.
23. Connell D.A., Ali K.E., Ahmad M., et. al.: Ultrasound-guided autologous blood injection for tennis elbow. Skeletal Radiol 2006; 35: pp. 371-377.
24. Mishra A., Pavelko T.: Treatment of chronic elbow tendinosis with buffered platelet-rich plasma. AJSM 2006; 34: pp. 1774-1778.
25. Kazemi M., Azma K., Tavana B., et. al.: Autologous blood versus corticosteroid local injection in the shortterm treatment of lateral elbow tendinopathy: a randomized clinical trial of efficacy. Am J Phys Med Rehabil 2010; 89: pp. 660-667.
26. Moriatis Wolf J., Ozer K., Scott F., et. al.: Comparison of autologous blood, corticosteroid, and saline injection in the treatment of lateral epicondylitis: a prospective, randomized, controlled multicenter study. J Hand Surg 2011; 36A: pp. 1269-1272.
27. Peerbooms J.C., Sluimer J., Bruijn D.J., et. al.: Positive effect of an autologous platelet concentrate in lateral epicondylitis in a double blind randomized controlled trial: platelet-rich plasma versus corticosteroid injection with a 1-year follow-up. Am J Sports Med 2010; 38: pp. 255-262.
28. Gosens T., Peerbooms J.C., van Laar W., et. al.: Ongoing positive effect of platelet-rich plasma versus corticosteroid injection in lateral epicondylitis. Am J Sports Med 2011; 39: pp. 1200-1208.
29. Krogh T.P., Fredberg U., Stengaard-Pedersen K., et. al.: Treatment of lateral epicondylitis with platelet-rich plasma, glucocorticoid, or saline: a randomized, double-blind, placebo-controlled trial. Am J Sports Med 2013; 41: pp. 625-635.
30. de Vos R.J., Weir A., van Schie H.T.M.: Platelet-rich plasma injection for chronic Achilles tendinopathy: a randomized controlled trial. JAMA 2010; 303: pp. 144-149.
31. Thanasas C., Papadimitriou G., Charalambidis C., et. al.: Platelet-rich plasma versus autologous whole blood for the treatment of chronic lateral elbow epicondylitis: A randomized controlled clinical trial. Am J Sports Med 2011; 20: pp. 1-5.
32. Platelet Rich Plasma: A Market Snapshot. http://www.docstoc.com/docs/47503668/Platelet-Rich-Plasma-A-Market-Snapshot .
33. Stenhouse G., Sookur P., Watson M.: Do blood growth factors offer additional benefit in refractory lateral epicondylitis? A prospective, randomized pilot trial of dry needling as a stand-alone procedure versus dry needling and autologous conditioned plasma. Skeletal Radiol 2013; 42: pp. 1515-1520.
34. Sathyamoorthy G.J., Kemp A., Rawal V.: Development and validation of an elbow score. Rheumatology 2004; 43: pp. 1434-1440.
35. Zigmond A.S., Snaith R.P.: The Hospital Anxiety and Depression Scale. Acta Psychiatr Scand 1983; 12: pp. 577-586.
36. Bjelland I., Dahl A.A., Haug T.T., et. al.: The validity of the Hospital Anxiety and Depression Scale. An updated literature review. J Psychosom Res 2002; 52: pp. 69-77.
37. Herrmann C.: International experiences with the Hospital Anxiety and Depression Scale—a review of validation data and clinical results. J Psychosom Res 1997; 42: pp. 17-41.
38. Pallant J.F., Bailey C.M.: Assessment of the structure of the Hospital Anxiety and Depression Scale in musculoskeletal patients. Health Qual Life Outcomes 2005; 3: pp. 82.
39. Ware J.E., Kosinski M., Keller S.D.: How to score the SF-12 physical and mental health summary scales.2nd ed.1995.The Health Institute, New England Medical CenterBoston