
Rationale and Objectives
The Resident Review Committee (RRC) recently changed the policy concerning first-year resident call. Our study is intended to evaluate whether the additional 6 months of training before a resident’s first call made a significant difference in the resident’s ability to provide patient care. To evaluate this, we assessed the discrepancy rates between preliminary interpretations made by residents and final reports by attendings.
Materials and Methods
All cross-sectional imaging interpreted by on-call residents (5 PM to 8 AM) during the first 6 months of call duties was reviewed for discrepant findings between the preliminary resident report and the final interpretation by an attending. Only major discrepancies were evaluated. A major discrepancy was defined as a change made to the resident preliminary report by an attending radiologist where a delay in communicating that finding had the potential to negatively affect clinical outcomes. Major discrepancy rates between groups were then compared.
Results
During the second 6 months of the 2008–2009 academic year, first-year residents interpreted 3331 studies. Fifty-nine of those were declared to be discrepancies after an attending over-read, a rate of 1.8%. During the first 6 months of the 2009–2010 academic year, second-year residents interpreted 4649 studies with 49 discrepancies, a rate of 1.0%. This difference is statistically significant ( P = .008).
Conclusions
The recent RRC policy change requiring 6 additional months of training before assuming independent on-call responsibilities has significantly decreased the major discrepancy rate at our institution.
The Resident Review Committee (RRC) has recently changed the policy concerning first-year residents taking call. Radiology residents are now required to complete 12 months of training before taking independent call. This is the second such change in the last 20 years. In 1990, a 6-month training requirement was introduced. The RRC feels that the in-service exam is an indicator of resident readiness for independent call, citing increasing raw scores as proof of improving ability on call .
Two national program surveys that polled program directors and chief residents demonstrated that the change was unpopular, with 66%–70% of respondents against the change . Protests stated that there was no proof that the extra 6 months of training would have a significant impact on patient care, with overall clinically significant discrepancy rates ranging from 0.3% to 10% .
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Materials and methods
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Table 1
Discrepancy Rates after 6 Months of Training
2008–2009n Discrepancies % Total 3331 59 1.8 Musculoskeletal 483 4 0.08 Neurology 887 7 0.08 Chest 755 9 1.2 Body 1206 32 2.6
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 2
Discrepancy Rates after 12 Months of Training
2009–2010n Discrepancies % Total 4649 49 1.0 Musculoskeletal 1056 11 1.0 Neurology 1594 18 1.1 Chest 856 9 1.0 Body 1156 11 1.0
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
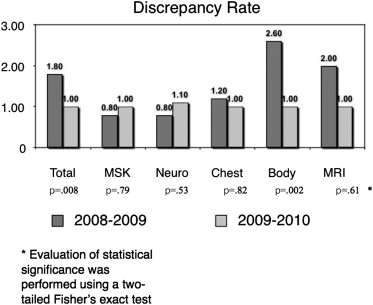
Table 3
Overall Resident Major Discrepancy Rates
Study Imaging Interpreted No. of Studies Major Discrepancies Our study All cross-sectional 16,043 1% Wechsler Body CT 598 1.2% Yoon Abdominal/pelvis CT 512 2.3% Roszler Cranial CT 289 2.0% Wysoki Cranial CT 419 1.7% Velmahos Trauma CT 383 5.0% Carney Body CT/US 928 0.5% Fillipi Neurologic MRI 361 4.2%
CT, computed tomography; US, ultrasound; MRI, magnetic resonance imaging.
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 4
Discrepancy Rates Broken Down by PGY
Study Exams PGY 2 PGY 3 PGY 4 PGY 5 Fellow Our study All cross-sectional 1.8% 1.0% 0.79% 0.48% NA Filippi Neurologic MRI 6.3% 2.8% 3.4% NA NA Ruchman All 1.5% 2.9% 3.3% 2.2% NA Wysoki Head CT 2.4% 0.0% 4.0% NA NA Wechsler Body CT NA 0.0% 7.8% NA 0.7% Erly Head CT 2.0% 1.0% 0.0% 0.0% NA
CT, computed tomography; MRI, magnetic resonance imaging; PGY, postgraduate year.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Acknowledgment
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Berger W., Gibson S., Drupinski E., et. al.: Proposed ACGME change in length of radiology residency training before independent call: results of a survery of program directors and chief medical residents. J Am Coll Radiol 2007; 4: pp. 595-601.
2. Gunderman R., Delaney L.: Should 12 months of training be required before diagnostic radiology residents take independent call? A survey of the association of program directors in radiology. J Am Coll Radiol 2007; 4: pp. 590-594.
3. Chung J.H., Strigel R.M., Chew A.R., et. al.: Overnight resident interpretation of torso CT at a level 1 trauma center: an analysis and review of the literature. Acad Radiol 2009; 16: pp. 1155-1160.
4. Sistrom C., Deitte L.: Factors affecting attending agreement with resident early readings of computed tomography and magnetic resonance imaging of the head, neck, and spine. Acad Radiol 2008; 15: pp. 934-941.
5. Ruchman R., Jaeger J., Wiggins E., et. al.: Preliminary radiology resident interpretations versus final attending radiologist interpretations and the impact on patient care in a community hospital. Am J Roentgenol 2007; 189: pp. 523-526.
6. Carney E., Kempf J., DeCarvalho V., et. al.: Preliminary interpretations of after-hours CT and sonography by radiology residents versus final interpretations by body imaging radiologists at a level 1 trauma center. Am J Roentgenol 2003; 181: pp. 367-373.
7. Wysoki M., Nassar C., Koenigsberg R., et. al.: Head trauma: CT scan interpretation by radiology residents versus staff radiologists. Radiology 1998; 208: pp. 125-128.
8. Yoon L., Haims A., Brink J., et. al.: Evaluation of an emergency radiology quality assurance program at a level 1 trauma center: abdominal and pelvic CT studies. Radiology 2002; 224: pp. 42-46.
9. Wechsler R., Spettel C., Kurtz A., et. al.: Effects of training and experience in interpretation of emergency body CT scans. Radiology 1996; 199: pp. 717-720.
10. Erly W., Berger W., Krupinski E., et. al.: Radiology resident evaluation of head CT scan orders in the emergency department. Am J Neuroradiol 2002; 23: pp. 103-107.
11. Filippi C., Schneider B., Burbank H., et. al.: Discrepancy rates of radiology resident interpretations of on-call neuroradiology MR imaging studies. Radiology 2008; 249: pp. 972-979.
12. Velmahos G.C., Fili C., Vasiliu P., et. al.: Around the-clock attending radiology coverage is essential to avoid mistakes in the care of trauma patients. Am Surg 2001; 67: pp. 1175-1177.
13. Roszler M.H., McCarroll K.A., Rashid T., et. al.: Resident interpretation of emergency computed tomographic scans. Invest Radiol 1991; 26: pp. 374-376.