
Rationale and Objectives
To assess radiologists’ perceptions of how the new Breast Density Notification Act (BDNA) of Pennsylvania would affect their breast density reporting and their actual reporting patterns after implementation.
Materials and Methods
Under an institutional review board–approved protocol, we surveyed 21 radiologists about how they believe the new law affected their breast density reporting patterns and analyzed actual changes for 16 respondents before and after the law took effect. Three hundred consecutive reports were assessed for each radiologist before and after the effective date. The distributions of reported density Breast Imaging Reporting and Data System (BI-RADS) (1–4) were compared using a type III test in the context of an ordinal mixed model accounting for between-reader variability and adjusting for age (PROC GLIMMIX, SAS, version 9.3) using a two-sided .05 significance level.
Results
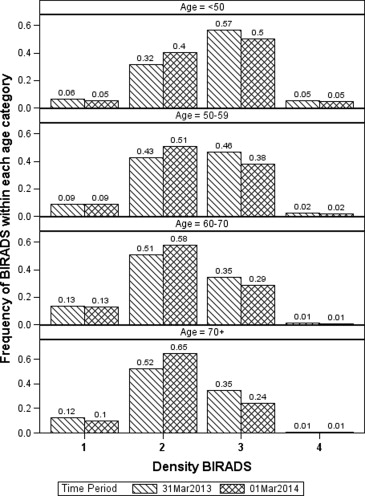
Seventeen radiologists responded to the survey; however, one retired shortly after responding. Of the 16 respondents, 56% (nine of 16) did not favor the law, 13% (two of 16) were in favor, and 31% (five of 16) were neutral. The fraction perceived that after implementation, they rated more, equally, or less frequently breasts as scattered fibroglandular densities (BI-RADS 2) versus heterogeneously dense rating (BI-RADS 3) was 50% (eight of 16), 44% (seven of 16), and 6% (one of 16), respectively. In practice, 44% (seven of 16) performed differently than their survey answers. Fourteen of 16 radiologists increased the frequency of reported BI-RADS 2 scores after BDNA implementation with seven having statistically significant ( P < .05) increases after adjusting for age differences.
Conclusions
Radiologists’ reporting patterns changed, at least for a short duration, after the new density reporting law and for some of the radiologists in an unexpected way.
Studies have shown that breast density is a strong breast cancer risk indicator . Two well-recognized approaches to assess breast density using mammograms were initially proposed and tested by Wolfe in 1976 and Pike in 1983 . Since then, many studies have investigated the correlation between mammographic tissue density and breast cancer risk . Some studies reported that women with mammographic high density have as much as four and six times the risk of developing breast cancer of age-matched women with low breast density . In addition, mammographic tissue density was also shown to be associated with a number of genetic risk factors (ie, BRCA1 and/or BRCA2 gene mutations ), as well as with family history of breast cancer . As a result, it is widely believed that mammographic density is an easily measured, assessable, important and likely heritable risk factor . With the belief that increased breast density constitutes an elevated risk for breast cancer and decreases sensitivity of mammography screening, 19 states enacted breast density notification laws as of July 2014. In Pennsylvania, the Breast Density Notification Act (BDNA) was signed into law in November 2013 and put into effect on February 1, 2014. This law requires mammography providers to notify women of their breast density, to raise their awareness of the associated elevated risk, if any, and to consult their physician regarding their care. Although breast density is a Breast Imaging Reporting and Data System (BI-RADS) requirement of the mammography report, radiologists were not required to notify patients of their assessed breast density. Therefore, in clinical practice, there was no direct implication associated with breast density assignment and/or reporting. Because the threshold for increased awareness for breast cancer risk and decreased mammography sensitivity is between scattered (BI-RADS rating 2) and heterogeneously dense (BI-RADS rating 3) ratings, additional/supplemental imaging is recommended to be considered for women diagnosed with heterogeneously and extremely dense breasts (BI-RADS rating 3 and 4). These two breast density groups constitute about 40% of the screening population . Hence, unlike the “high-risk” group of women who are already recommended to undergo breast magnetic resonance imaging, the reporting distribution between these two groups (ie, BI-RADS 2 and 3) that is intended to differentiate between women at “average risk” and women at “intermediate risk,” may substantially affect imaging practices and resource utilization . Higher costs to patients and providers may occur based on reactions to the breast density notifications for those patients diagnosed with heterogeneously or extremely dense breast tissue, and costs could further increase if indeed radiologists’ reporting patterns change toward a greater density rating. Shifting the rating toward a lesser density may result in circumventing the intent of the law, which is intended to advise women with denser breasts to discuss with their physicians the possible implementation of supplemental screening tests. Neither radiologists’ perceptions of the impact of the new law requiring the reporting of breast density nor their actual reporting patterns during clinical practice have been studied to date. Therefore, during the first month after the implementation of the BDNA that went into effect in February 1, 2014, in Pennsylvania, we presented a simple survey to our women’s imaging radiologists as to their attitude about the law and their expectations of whether it has affected, or not, their density reporting patterns and then compared their responses to their actual reporting patterns.
Materials and methods
Under an institutional review board–approved Health Insurance Portability and Accountability Act HIPAA-compliant protocol with waiver of a written consent, we sent a survey via email to a total of 21 Mammography Quality Standards Act MQSA-qualified academic breast imaging radiologists at our institution with 4–34 years of experience in interpreting mammograms. The survey’s purpose was to gain knowledge of the radiologists’ attitudes regarding the new density law enacted in Pennsylvania and if they think they have changed (or would change) the way they report breast density after implementation of the new law. The email was sent a month after the law was put into effect on March 4, 2014, by the research coordinator and included a brief introductory paragraph explaining the purpose of the research, the voluntary nature of the survey, and the individual’s results will remain deidentified to the investigators. The actual survey included the following two questions: 1) Do you believe the new law has changed the way you rate breast density between scattered fibroglandular densities versus heterogeneously dense? Specifically, do you believe you rate density BI-RADS 2 (“scattered” fibroglandular tissue): A. Less, B. Equal, or C. More; and 2) “Were you in favor of enacting this law?” (allowed responses were no, yes, or neutral.) Seventeen radiologists responded to the survey; however, one radiologist retired shortly after responding to the survey. Therefore, there were a total of 16 radiologists who completed the survey and for whom we reviewed their breast density reporting distribution of ratings before and after the implementation of the law.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 1
Frequencies of BI-RADS 2 Scores and Age Distribution by Radiologist and Subgroups of Subjective Impression Before and After Implementing the BDNA
Survey Response Readers Total Before (Pre) the BDNA After (Post) the BDNA Difference Average Age of Population Cases Reported as BI-RADS 2 Rate ∗ Average Age of Population Cases Reported as BI-RADS 2 Rate ∗ Rate Difference † P Value ‡ No change (“equal”) 1 300 58.0 99 0.33 59.7 117 0.39 0.06 .224 2 300 56.6 189 0.63 56.1 177 0.59 −0.04 .346 3 300 67.5 173 0.58 66.9 219 0.73 0.15<.001 4 300 55.9 110 0.37 57.0 136 0.45 0.09 .056 5 300 57.3 155 0.52 56.3 141 0.47 −0.05 .270 6 300 56.1 132 0.44 57.0 153 0.51 0.07 .123 7 300 55.5 61 0.20 56.8 135 0.45 0.25<.001 All (“equal”) 2100 58.1 919 0.44 58.6 1078 0.51 0.08 .090 Less frequently (“less”) 8 300 55.6 116 0.39 57.4 184 0.61 0.23<.001 More frequently (“more”) 9 300 56.8 162 0.54 58.0 168 0.56 0.02 .755 10 300 58.6 142 0.47 59.9 152 0.51 0.03 .539 11 300 58.8 142 0.47 58.2 213 0.71 0.24<.001 12 300 57.0 141 0.47 58.4 184 0.61 0.14.001 13 300 56.9 131 0.44 59.7 144 0.48 0.04 .624 14 300 55.1 127 0.42 57.9 149 0.50 0.07 .211 15 300 56.6 97 0.32 58.5 126 0.42 0.10.022 16 300 56.8 97 0.32 57.1 123 0.41 0.09.029 All (“more”) 2400 57.1 1039 0.43 58.5 1259 0.52 0.09.010 Overall480057.420740.4358.425210.530.09.02
BDNA, Breast Density Notification Act; BI-RADS, Breast Imaging Reporting and Data System.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Conclusion
Get Radiology Tree app to read full this article<
References
1. Amir E., Freedman O.C., Seruga B., et. al.: Assessing women at high risk of breast cancer: a review of risk assessment models. JNCI 2010; 102: pp. 680-691.
2. Tice J.A., Cummings S.R., Smith-Bindman R., et. al.: Using clinical factors and mammographic breast density to estimate breast cancer risk: development and validation of a new predictive model. Ann intern Med 2008; 148: pp. 337-347.
3. Wolfe J.N.: Breast patterns as an index of risk for developing breast cancer. Am J Roentgenol 1976; 126: pp. 1130-1139.
4. Pike M.C., Krailo M.D., Henderson B.E., et. al.: ‘Hormonal’ risk factors, ‘breast tissue age’ and age-incidence of breast cancer. Nature 1983; 303: pp. 767-770.
5. Boyd N.F., Martin L.J., Bronskill M., et. al.: Breast tissue composition and susceptibility to breast cancer. J Natl Cancer Inst 2010; 102: pp. 1224-1237.
6. McCormack V.A., dos Santos Silva I.: Breast density and parenchymal patterns as markers of breast cancer risk: a meta-analysis. Cancer Epidemiol Biomarkers Prev 2006; 15: pp. 1159-1169.
7. Boyd N.F., Martin I.J., Stone J., et. al.: Mammographic densities as a marker of human breast cancer risk and their use in chemoprevention. Curr Oncol Rep 2001; 3: pp. 314-321.
8. Brisson J., Diorio C., Masse B.: Wolfe’s parenchymal pattern and percentage of the breast with mammographic densities: redundant or complementary classifications?. Cancer Epidemiol Biomarkers Prev 2003; 12: pp. 728-732.
9. Li T., Sun L., Miller N., et. al.: The association of measured breast tissue characteristics with mammographic density and other risk factors for breast cancer. Cancer Epidemiol Biomarkers Prev 2005; 14: pp. 343-349.
10. Vachon C.M., Sellers T.A., Carlson E.E., et. al.: Strong evidence of a genetic determinant for mammographic density, a major risk factor for breast cancer. Cancer Res 2007; 67: pp. 8412-8418.
11. Martin L.J., Melnichouk O., Guo H., et. al.: Family history, mammographic density, and risk of breast cancer. Cancer Epidemiol Biomarkers Prev 2010; 19: pp. 456-463.
12. Tice J.A., Cummings S.R., Ziv E., et. al.: Mammographic breast density and the Gail model for breast cancer risk prediction in screening population. Breast Cancer Res Treat 2005; 94: pp. 115-122.
13. Mitchell G., Antoniou A.C., Warren R., et. al.: Mammographic density and breast cancer risk in BRCA1 and BRCA2 mutation carriers. Cancer Res 2006; 66: pp. 1866-1872.
14. Stomper P.C., D’Souza D.J., DiNitto P.A., et. al.: Analysis of parenchymal density on mammograms in 1353 women 25–79 years old. AJR 1996; 167: pp. 1261-1265.
15. Ho J.M., Jafferjee N., Covarrubias G.M., et. al.: Dense breasts: a review of reporting legislation and available supplemental screening options. AJR Am J Roentgenol 2014; 203: pp. 449-456.
16. Work M.E., Reimers L.L., Quante A.S., et. al.: Changes in mammographic density over time in breast cancer cases and women at high risk for breast cancer. Int J Cancer 2014; 135: pp. 1740-1744.
17. Boyd N.F., Byng J.W., Jong R.A., et. al.: Quantitative classification of mammographic densities and breast cancer risk: results from the Canadian National Breast Screening Study. J Natl Cancer Inst 1995; 87: pp. 670-675.
18. Byng J.W., Boyd N.F., Fishell E., et. al.: Automated analysis of mammographic densities. Phys Med Biol 1996; 41: pp. 909-923.
19. Byng J.W., Boyd N.F., Fishell E., et. al.: The quantitative analysis of mammographic densities. Phys Med Biol 1994; 39: pp. 1629-1638.
20. Gweon H.M., Youk J.H., Kim J.A., et. al.: Radiologist assessment of breast density by BI-RADS categories versus fully automated volumetric assessment. AJR Am J Roentgenol 2013; 201: pp. 692-697.
21. Tagliafico A., Tagliafico G., Tosto S., et. al.: Mammographic density estimation: comparison among BI-RADS categories, a semi-automated software and a fully automated one. Breast 2009; 18: pp. 35-40.