
Rationale and Objectives
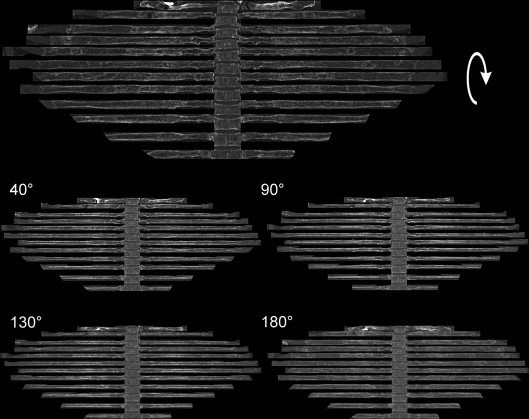
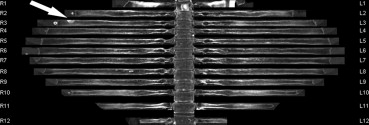
To evaluate the performance of a dedicated computed tomography (CT) software called “bone reading” generating rib unfolded images for improved detection of rib metastases in patients with lung cancer in comparison to readings of 5- and 1-mm axial CT images and 18 F-Fluordeoxyglucose positron emission tomography/computed tomography (FDG-PET/CT).
Materials and Methods
Ninety consecutive patients who underwent 18 F-FDG-PET/CT and chest CT scanning between 2012 and 2014 at our institution were analyzed retrospectively. Chest CT scans with 5- and 1-mm slice thickness were interpreted blindly and separately focused on the detection of rib metastases (location, number, cortical vs. medullary, and osteoblastic vs. sclerotic). Subsequent image analysis of unfolded 1 mm–based CT rib images was performed. For all three data sets the reading time was registered. Finally, results were compared to those of FDG-PET. Validation was based on FDG-PET positivity for osteolytic and mixed osteolytic/osteoblastic focal rib lesions and follow-up for sclerotic PET-negative lesions.
Results
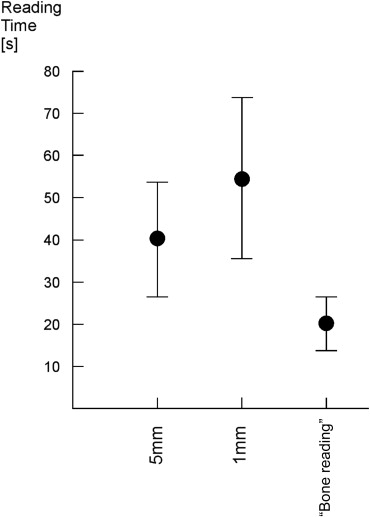
A total of 47 metastatic rib lesions were found on FDG-PET/CT plus another 30 detected by CT bone reading and confirmed by follow-up CT. Twenty-nine lesions were osteolytic, 14 were mixed osteolytic/osteoblastic, and 34 were sclerotic. On a patient-based analysis, CT (5 mm), CT (1 mm), and CT (1-mm bone reading) yielded a sensitivity, specificity, and accuracy of 76.5/97.3/93, 81.3/97.3/94, and 88.2/95.9/92, respectively. On segment-based (unfolded rib) analysis, the sensitivity, specificity, and accuracy of the three evaluations were 47.7/95.7/67, 59.5/95.8/77, and 94.8/88.2/92, respectively. Reading time for 5 mm/1 mm axial images and unfolded images was 40.5/50.7/21.56 seconds, respectively.
Conclusions
The use of unfolded rib images in patients with lung cancer improves sensitivity and specificity of rib metastasis detection in comparison to 5- and 1-mm CT slice reading. Moreover, it may reduce the reading time.
Lung cancer is one of the most common types of cancer in the world with steadily increasing incidence, and it has one of the highest cancer-related death rates . Bone metastases are found in 20%–40% of patients with lung cancer at the initial diagnosis . Accurate staging of these patients has prognostic and therapeutic consequences as disseminated disease generally implies systemic, palliative therapy. Moreover, skeletal-related events are frequent complications in these patients . Bone metastases can involve any skeletal site, but the spine and the ribs are most frequently impacted as they represent the reservoir of hematopoietic bone marrow in adults, which is known to be better vascularized . Most skeletal metastases are primarily osteolytic or mixed osteolytic/osteoblastic, whereas some are sclerotic . Depending on which computed tomography (CT) imaging protocol is used, more than half of the bone metastases are already visible on anatomical (CT) imaging . Nevertheless, partial volume average and inadequate spatial resolution filters can mask some of these lesions. Additionally, some metastases are temporarily not accompanied by evident bone destruction and are therefore depicted only in bone marrow imaging using bone scintigraphy, magnetic resonance imaging, or FDG-PET .
Inside the thoracic cage, rib metastases are generally difficult to identify on axial images because of their complex configuration with irregular surfaces and borders and, in part, a complex twisting course. They are therefore displayed only in small sections on CT. Moreover, there are consistent differences in the configuration and course between the upper two ribs and the others as well as between the so-called true and the false ribs. Finally, traumatic incidents with consequent rib fractures are frequent, and therefore focal sclerotic lesions can sometimes be challenging for the radiologist.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Materials and methods
Subjects
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Imaging Techniques
CT Imaging Data Acquisition
Get Radiology Tree app to read full this article<
Standard of Reference
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Image Analysis
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
FDG-PET Image Analysis
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results
Patient Population
Get Radiology Tree app to read full this article<
CT Reading Results
Get Radiology Tree app to read full this article<
Table 1
Lesion Characteristics
Lesion Characteristic Lesion Number Mean Lesion Size ± Standard Deviation (cm) Lesion Location Caput Collum Corpus Osteolytic 29 1.64 ± 1.44 0 4 25 Osteoblastic 34 1.16 ± 1.15 0 2 32 Mixed 14 1.64 ± 1.23 1 2 11
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Lesion Characteristics and Distribution
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 2
Lesion Distribution Along and Inside the Ribs
1st/2nd Rib 3rd–9th Rib 10th–12th Rib Total Cortical 4 21 4 29 Medullary 6 40 2 48
Get Radiology Tree app to read full this article<
Analysis on Per-Patient Basis
Get Radiology Tree app to read full this article<
Table 3
Analysis of Rib Metastases on Per-Patient Basis
Total 5 mm 1 mm Bone Reading Sensitivity 76.47% 81.25% 88.24% Specificity 97.26% 97.3% 95.89% Accuracy 0.93 0.94 0.94
Get Radiology Tree app to read full this article<
Analysis on Per-Lesion Basis
Get Radiology Tree app to read full this article<
Table 4
Analysis of Rib Metastases on Per-Lesion Basis Considering Also Lesion’s Size
Total 5 mm 1 mm Bone Reading Sensitivity 47.69% 59.46% 94.81% Specificity 95.65% 95.77% 88.24% Accuracy 0.67 0.77 0.92
5 mm 1 mm Bone Reading <8 mm ≥8 mm <8 mm ≥8 mm <8 mm ≥8 mm Sensitivity 11.53% 57.14% 25.0% 73.47 89.29% 100% Specificity 93.3% 97.5% 91.67% 97.5% 85.19% 90.24%
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Analysis of FDG-PET–Negative Lesions
Get Radiology Tree app to read full this article<
Table 5
Analysis of 18 F-FDG-PET Negative Rib Metastases
Total Mean Size (cm) Localization Medullary Cortical Osteolytic 0.78 ± 0.24 2 11 Osteoblastic 0.61 ± 0.25 9 8 Mixed 0.74 ± 0.32 3 2
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Acknowledgments
Get Radiology Tree app to read full this article<
Appendix
FDG-PET/CT imaging data
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Parkin D.M., Bray F., Ferlay J., et. al.: Global cancer statistics, 2002. CA Cancer J Clin 2005; 55: pp. 74-108.
2. Min J.W., Um S.W., Yim J.J., et. al.: The role of whole-body FDG PET/CT, Tc 99m MDP bone scintigraphy, and serum alkaline phosphatase in detecting bone metastasis in patients with newly diagnosed lung cancer. J Korean Med Sci 2009; 24: pp. 275-280.
3. Tsuya A., Kurata T., Tamura K., et. al.: Skeletal metastases in non-small cell lung cancer: a retrospective study. Lung Cancer 2007; 57: pp. 229-232.
4. Oster G., Lamerato L., Glass A.G., et. al.: Natural history of skeletal-related events in patients with breast, lung, or prostate cancer and metastases to bone: a 15-year study in two large US health systems. Support Care Cancer 2013; 21: pp. 3279-3286.
5. Kagohashi K., Satoh H., Ishikawa H., et. al.: Bone metastasis as the first manifestation of lung cancer. Int J Clin Pract 2003; 57: pp. 184-186.
6. Maccauro G., Spinelli M.S., Mauro S., et. al.: Physiopathology of spine metastasis. Int J Surg Oncol 2011; 2011: pp. 107969.
7. Weiss L., Haydock K., Pickren J.W., et. al.: Organ vascularity and metastatic frequency. Am J Pathol 1980; 101: pp. 101-113.
8. Nakamoto Y., Osman M., Wahl R.L.: Prevalence and patterns of bone metastases detected with positron emission tomography using F-18 FDG. Clin Nucl Med 2003; 28: pp. 302-307.
9. A learning based deformable template matching method for automatic rib centreline extraction and labeling in CT images. Available at: http://ieeexplore.ieee.org/xpl/articleDetails.jsp?reload=true&tp=&arnumber=6247774&url=http%3A%2F%2Fieeexplore.ieee.org%2Fxpls%2Fabs_all.jsp%3Farnumber%3D6247774 . Accessed November 11, 2014.
10. Moses W.W.: Fundamental limits of spatial resolution in PET. Nucl Instrum Methods Phys Res A 2011; 648: pp. 236-240.
11. Toth D.F., Töpker M., Mayerhöfer M.E., et. al.: Rapid detection of bone metastasis at thoracoabdominal CT: accuracy and efficiency of a new visualization algorithm. Radiology 2014; 270: pp. 825-833.
12. Evangelista L., Panunzio A., Polverosi R., et. al.: Early bone marrow metastasis detection: the additional value of FDG-PET/CT vs. CT imaging. Biomed Pharmacother 2012; 66: pp. 448-453.
13. Fogelman I., Cook G., Israel O., et. al.: Positron emission tomography and bone metastases. Semin Nucl Med 2005; 35: pp. 135-142.
14. Liu N., Ma L., Zhou W., et. al.: Bone metastasis in patients with non-small cell lung cancer: the diagnostic role of F-18 FDG PET/CT. Eur J Radiol 2010; 74: pp. 231-235.
15. Qu X., Huang X., Yan W., et. al.: A meta-analysis of 18 FDG-PET-CT, 18 FDG-PET, MRI and bone scintigraphy for diagnosis of bone metastases in patients with lung cancer. Eur J Radiol 2012; 81: pp. 1007-1015.
16. Ozülker T., Küçüköz Uzun A., Ozülker F., et. al.: Comparison of (18)F-FDG-PET/CT with (99m)Tc-MDP bone scintigraphy for the detection of bone metastases in cancer patients. Nucl Med Commun 2010; 31: pp. 597-603.
17. Choi H.S., Yoo I.R., Park H.L., et. al.: Role of 18 F-FDG PET/CT in differentiation of a benign lesion and metastasis on the ribs of cancer patients. Clin Imaging 2014; 38: pp. 109-114.
18. Cook G.J., Fogelman I.: The role of positron emission tomography in the management of bone metastases. Cancer 2000; 88: pp. 2927-2933.
19. Gruden J.F., Ouanounou S., Tigges S., et. al.: Incremental benefit of maximum-intensity-projection images on observer detection of small pulmonary nodules revealed by multidetector CT. AJR Am J Roentgenol 2002; 179: pp. 149-157.