
Rationale and Objectives
Radiology residents must acquire dictation and reporting skills to meet Accreditation Council for Graduate Medical Examination requirements and provide optimal patient care. Historically, these skills have been taught informally and vary between institutions and among radiologists. A structured curriculum improves resident report quality when using a quantitative grading scheme. This study describes the implementation of such a curriculum and evaluates its utility in tracking resident progress.
Materials and methods
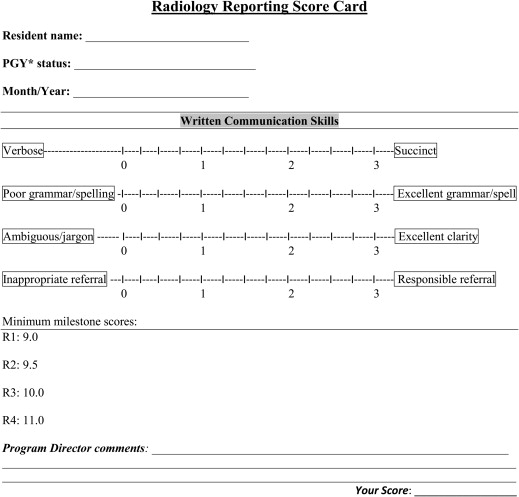
We implemented a three-stage reporting curriculum in our diagnostic radiology residency program in 2009. Stages 1 and 2 involve instruction and formative feedback composed of suggestions for improvement in a 360° format from faculty, peers, and others within the resident’s sphere of influence. The third stage involves individual, biannual, written feedback with scored reports specifically assessing four categories: succinctness, spelling/grammar, clarity, and responsible referral. Biannual scores were collected from 2009 to 2013, sorted by year of residency training (R1 to R4), and average training level scores were statistically compared.
Results
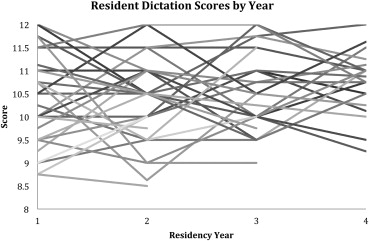
Review of 1500 reports over a 4-year period yielded a total of 153 scores: 54, 36, 29, and 34 from R1, R2, R3, and R4 residents, respectively. The mean (standard deviation) scores for R1, R2, R3, and R4 residents were 10.20 (1.06), 10.25 (0.81), 10.5 (0.74), and 10.75 (0.69), respectively. Post hoc analysis identified significant differences between R1 and R4 residents ( P = .012) and R2 and R4 residents ( P = .009).
Conclusions
Residents’ reporting scores showed significant improvement over the course of their residency training. This indicates that there may be a benefit in using an organized reporting curriculum to track resident progress in producing reports that may improve patient care.
The Accreditation Council of Graduate Medical Education (ACGME) has recently released the Next Accreditation System, which requires the individual specialties to develop specific milestones that residents should meet at expected intervals throughout their training within the six core competencies . Two of the six core competencies outlined by the ACGME are patient care/technical skills and interpersonal/communication skills . The graduating resident is expected to meet milestone level 4 of these core competencies. For example, in diagnostic radiology under interpersonal/communication skills, the resident “communicates complex and difficult information, such as errors, complications, adverse events, and bad news” .
Radiologists provide quality patient care by communicating succinct, clear, and accurate information to referring physicians . This can be in the form of the radiology report and through direct consultation with clinicians on a specific patient’s imaging needs. Recent evidence suggests primary care physicians are generally very satisfied with radiology reports, but they differ in what aspects of the report they value most . Because the radiology report is the primary and most frequent mode of communication, it is important for radiology residents to complete their training with competent effective dictation and reporting skills. Furthermore, it is notable that improper communication is the second most common reason for malpractice lawsuits and can lead to significant patient and referring physician dissatisfaction with care . Thus, obtaining excellent communication skills may help avoid malpractice lawsuits, improve patient care, and indirectly lower health-care costs.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Materials and Methods
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 1
Outline of Online Reporting Modules ∗
Module 1: Preliminary Considerations Section 1: Key findings Section 2: Clinical urgency (triage) Section 3: General concepts Module 2: Components of a Report Section 1: Demographics Section 2: Indication for study Section 3: Technical procedural Section 4: Comparison/supplementary Section 5: Body Section 6: Summary/impression Module 3: Communication Outside of the Report Section 1: Personal/telephone contact Section 2: Conferences Section 3: Patient communication Section 4: Contact technology
Get Radiology Tree app to read full this article<
Table 2
Suggested Words and Phrases to Avoid with Rationale for Avoidance
1. Vague or unclear jargon ∗ that can be replaced with more descriptive anatomic terms a. Aspect b. Visible c. Non-specific 2. Vague or ambiguous terms used in place of the word “normal” a. Negative (can mean bad or normal) b. Intact c. Maintained or well-maintained d. Preserved e. Unremarkable 3. Statements with no information that refer readers back to the body of the report or to prior reports a. Stating something is unchanged without describing its current appearance (e.g., lines are unchanged)—This is the same as saying “read the prior report” b. As above in an impression—This is the same as saying “read my report” c. Description of “stable finding” without further description as normal or abnormal 4. Vague reference to prior examinations without specifying the date of study 5. Vague description of study limitations or findings without explanation of importance a. Pulmonary vascular congestion without stating which vessels are involved b. Degenerative disease without further describing location or severity c. Vascular calcification without specifying location or severity 6. Phrases lengthening the report that can be omitted without changing the report meaning a. Appearance of b. Evidence of 7. Words and phrases that imply uncertainty, doubt, and insecurity without explanation a. Essential, essentially b. Relative, relatively c. Gross or grossly 8. Vague qualitative, judgment, or statistical words and phrases a. Quite b. Some c. Good d. Satisfactory e. Significant 9. Redundant or incorrect anatomical descriptions a. Bilateral lungs, orbits, or kidneys—This is redundant as these organs are always bilateral b. Lung fields—No such anatomy 10. Vague recommendations or lack of communication of recommendations a. Clinical correlation recommended b. Additional imaging recommended without explanation as to why c. Additional imaging recommended without documenting clinician communication 11. Repetitive use of phrase “There are” or “there is” at the beginning of all sentences
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Table 3
Descriptive Statistics
Year Number Minimum Maximum Mean SD R1 54 8.5 12 10.20 1.06 R2 36 8.5 11.88 10.26 0.81 R3 29 9 12 10.47 0.74 R4 34 9.25 12 10.77 0.69
R1, radiology training year 1; R2, radiology training year 2; R3, radiology training year 3; R4, radiology training year 4; SD, standard deviation.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
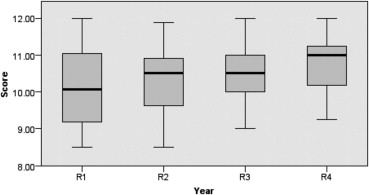
Table 4
Mann–Whitney U Comparisons to Identify Significant Differences between Means
Years Mann–Whitney U Wilcoxon W__Z__P value R1–R2 918 2403 −0.45 .655 R1–R3 659.5 2144.5 −1.19 .236 R1–R4 627 2112 −2.51 .012 R2–R3 468.5 1134.5 −0.71 .477 R2–R4 393.5 1059.5 −2.60 .009 R3–R4 370.5 805.5 −1.70 .088
R1, radiology training year 1; R2, radiology training year 2; R3, radiology training year 3; R4, radiology training year 4.
P value defined as significant if < 0.05.
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 5
Summary of Prior Studies Assessing Radiology Communication and Reporting Skills: Methods Used and Results
Study Method Results Williamson et al., 2002 An Objective Structured Clinical Examination (OSCE)–assessed communication skills across levels of education Reporting skills improved after OSCE with increasing level of training in the program Donnelly and Strife, 2006 Detailed feedback reports focusing on professionalism and communication Found benefit in providing a professionalism booklet, providing feedback on performance Woodfield and Mainiero, 2008 Assessed reporting and communication learning objectives with pre- and postlecture tests Found significant improvement in test scores following a didactic lecture Buchmann et al., 2008 Residents are required to identify a systems problem and propose a solution Residents were able to learn systems-based practice concepts by recognizing system errors and offering a solution
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Acknowledgments
Get Radiology Tree app to read full this article<
References
1. ACGME-Common program requirements. Available at: http://www.acgme.org/acgmeweb/Portals/0/PFAssets/ProgramRequirements/CPRs2013.pdf . Accessed July 27, 2013.
2. Nasca T.J., Philibert I., Brigham T., et. al.: The next GME accreditation system—rationale and benefits. N Engl J Med 2012; 366: pp. 1051-1056.
3. ACGME, ABR. The Diagnostic Radiology Milestone Project. Available at: http://www.acgme-nas.org/assets/pdf/Milestones/DiagnosticRadiologyMilestones.pdf . Accessed July 27, 2013.
4. UMKC diagnostic radiology residency manual and curriculum 2013-14. Available at: http://med.umkc.edu/docs/radiology/Diagnostic_Radiology_Residency_Manual.pdf . Accessed July 28, 2013.
5. Gunn A.J., Sahani D.V., Bennett S.E., et. al.: Recent measures to improve radiology reporting: perspectives from primary care physicians. J Am Coll Radiol Jacr 2013 Feb; 10: pp. 122-127.
6. Berlin L.: Failure of radiologic communication: An increasing cause of malpractice litigation and harm to patients. Appl Radiol 2010; 39: pp. 1-2.
7. Cascade P.N., Berlin L.: Malpractice issues in radiology. American College of Radiology Standard for Communication. Ajr Am J Roentgenol 1999 Dec; 173: pp. 1439-1442.
8. Hall F.M.: Language of the radiology report: primer for residents and wayward radiologists. Ajr Am J Roentgenol 2000 Nov; 175: pp. 1239-1242.
9. Radiology reporting templates. Available at: http://www.radreport.org/index.php . Accessed July 27, 2013.
10. Johnson A.J., Chen M.Y., Swan J.S., et. al.: Cohort study of structured reporting compared with conventional dictation. Radiology 2009 Oct; 253: pp. 74-80.
11. Johnson A.J., Chen M.Y., Zapadka M.E., et. al.: Radiology report clarity: a cohort study of structured reporting compared with conventional dictation. J Am Coll Radiol Jacr 2010 Jul; 7: pp. 501-506.
12. Department of Health and Human Services. Code of Federal Regulations 2009. Available at: http://www.hhs.gov/ohrp/policy/ohrpregulations.pdf . Accessed July 27, 2013.
13. ACR Practice guideline for communication of diagnostic imaging findings. 2010. Available at: http://www.acr.org/∼/media/ACR/Documents/PGTS/guidelines/Comm_Diag_Imaging.pdf . Accessed July 27, 2013.
14. Lanier L, Sistrom C, Rathe, R. Curriculum in radiology reporting. Available at: http://protocols.xray.ufl.edu/live_crr/home/home.php . Accessed July 27, 2013.
15. Seltzer S.E., Kelly P., Adams D.F., et. al.: Expediting the turnaround of radiology reports: use of total quality management to facilitate radiologists’ report signing. Ajr Am J Roentgenol 1994 Apr; 162: pp. 775-781.
16. Morgan M.B., Branstetter B.F., Lionetti D.M., et. al.: The radiology digital dashboard: effects on report turnaround time. J Digit Imaging 2008 Mar; 21: pp. 50-58.
17. Langlotz C.P.: Structured radiology reporting: are we there yet?. Radiology 2009 Oct; 253: pp. 23-25.
18. RSNA reporting initiative. Available at: http://www.rsna.org/Reporting_Initiative.aspx . Accessed July 27, 2013.
19. Kahn C.E., Langlotz C.P., Burnside E.S., et. al.: Toward best practices in radiology reporting. Radiology 2009 Sep 1; 252: pp. 852-856.
20. Dunnick N.R., Langlotz C.P.: The radiology report of the future: a summary of the 2007 Intersociety Conference. J Am Coll Radiol 2008 May; 5: pp. 626-629.
21. Sistrom C.L., Langlotz C.P.: A framework for improving radiology reporting. J Am Coll Radiol 2005 Feb; 2: pp. 159-167.
22. Williamson K.B., Steele J.L., Gunderman R.B., et. al.: Assessing radiology resident reporting skills. Radiology 2002 Dec; 225: pp. 719-722.
23. Donnelly L.F., Strife J.L.: Establishing a program to promote professionalism and effective communication in radiology. Radiology 2006 Mar; 238: pp. 773-779.
24. Woodfield C.A., Mainiero M.B.: Radiology resident dictation instruction: effectiveness of the didactic lecture. J Am Coll Radiol Jacr 2008 Jul; 5: pp. 842-846.
25. Buchmann R.F., Deloney L.A., Donepudi S.K., et. al.: Development and implementation of a systems-based practice project requirement for radiology residents. Acad Radiol 2008 Aug; 15: pp. 1040-1045.
26. Coakley F.V., Liberman L., Panicek D.M.: Style guidelines for radiology reporting: a manner of speaking. Ajr Am J Roentgenol 2003 Feb; 180: pp. 327-328.
27. Fratt L. The referring physician’s wish list: What clinicians need from radiologists. 2011. Available at: http://www.healthimaging.com/index.php?option=com_articles&view=article&id=30855:the-referring-physicians-wish-list-what-clinicians-need-from-radiologists . Accessed July 27, 2013.
28. Berlin L.: Pitfalls of the vague radiology report. Ajr Am J Roentgenol 2000 Jun; 174: pp. 1511-1518.