
Highlights
Epicardial fat volume is independently associated with the presence and severity of systemic sclerosis.
Extrapericardial fat volume is only associated with the presence of systemic sclerosis.
Coronary artery calcification is not independently associated with systemic sclerosis.
Rationale and Objectives
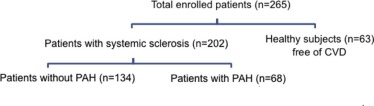
The study aimed to determine if intrathoracic fat volumes are associated with the presence and severity of systemic sclerosis (SSc), defined by the presence of pulmonary arterial hypertension (PAH).
Materials and Methods
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Conclusion
Get Radiology Tree app to read full this article<
Introduction
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Materials and Methods
Study Design
Get Radiology Tree app to read full this article<
Study Population
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
CT Technique
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
CT Image Reconstruction, Fat Measurement Technique, and Postprocessing
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results
Baseline Characteristics
Get Radiology Tree app to read full this article<
TABLE 1
(a) Baseline Characteristics of Controls and Patients with Systemic Sclerosis and (b) Baseline Characteristics of Systemic Sclerosis Patients with and without Systemic Sclerosis-Associated Pulmonary Arterial Hypertension
(a) Controls ( N = 63) Systemic Sclerosis ( N = 202)P Value Age (years) 49 ± 11 55 ± 13 0.0004 § Heart rate \* (bpm) 62 ± 11 79 ± 15 <0.0001 § Weight (kg) 82 ± 16 74 ± 19 0.0004 § Height (cm) 172 ± 12 164 ± 10 <0.0001 § BMI (kg/m 2 ) 29 ± 5 27 ± 6 0.0467 § BSA (m 2 ) 1.9 ± 0.2 1.8 ± 0.2 0.0005 § Women, % (n) 52 (33) 79 (159) <0.0001 § CAD, % (n) 0 (0) 10 (21) 0.0055 § ILD, % (n) 0 (0) 63 (124) <0.0001 § Hyperlipidemia, % (n) 0 (0) 23 (46) <0.0001 § Ever smoker † , % (n) 1.6 (1) 42 (80) <0.0001 § CAC 0 (0) 61 (124) <0.0001 § Epicardial fat (cm 3 ) 59 (30–81) 154 (120–202) <0.0001 § Extrapericardial fat (cm 3 ) 79 (48–96) 95 (68–141) <0.0001 § Intrathoracic fat (cm 3 ) 139 (79–179) 268 (199–341) <0.0001 §
(b) Systemic Sclerosis, No PAH ( N = 134) Systemic Sclerosis-Associated PAH ( N = 68)P Value Age (years) 51 ± 14 63 ± 10 <0.0001 § Heart rate (bpm) 80 ± 15 78 ± 15 0.34 Weight (kg) 75 ± 19 71 ± 18 0.17 Height (cm) 165 ± 10 162 ± 9 0.02 § BMI (kg/m 2 ) 27 ± 6 27 ± 6 0.89 BSA (m 2 ) 1.8 ± 0.2 1.8 ± 0.2 0.08 Women, % (n) 77 (103) 82 (56) 0.37 CAD, % (n) 4 (6) 22 (15) 0.0001 § ILD, % (n) 55 (74) 78 (50) 0.002 § Hyperlipidemia, % (n) 15 (20) 38 (26) 0.0002 § Ever Smoker ‡ , % (n) 41 (51) 44 (29) 0.67 CAC 51 (68) 82 (56) <0.0001 § Epicardial fat (cm 3 ) 145 (112–195) 178 (143–225) 0.0003 § Extrapericardial fat (cm 3 ) 90 (65–128) 113 (77–160) 0.002 § Intrathoracic fat (cm 3 ) 243 (171–314) 307 (224–384) 0.0003 §
BMI, body mass index; bpm, beats per minute; BSA, body surface area; CAC, coronary arterial calcification; CAD, coronary artery disease; ILD, interstitial lung disease; PAH, pulmonary arterial hypertension; SSc, systemic sclerosis.
Fat volumes are presented as medians and interquartile range (IQR). Other continuous variables are presented as means and standard deviations when appropriate. Categorical variables are presented as a percentage (%).
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
ITFV and Clinical Characteristics in Patients with SSc
Get Radiology Tree app to read full this article<
TABLE 2
Associations Between Epicardial Fat Volume and Clinical Variables in Patients with Systemic Sclerosis Using General Linear Model
Fat Volumes (cm 3 ) Epicardial Fat Volume Extrapericardial Fat Volume Estimate difference ± SE_P_ Value Estimate difference ± SE_P_ Value Age 1.39 ± 0.3 <0.0001 1.8 ± 0.3 <0.0001 ‡ Multivariate \* 1.1 ± 0.3 0.001 1.67 ± 0.3 <0.0001 ‡ Gender 31.6 ± 10.3 0.002 ‡ 62.1 ± 10.3 <0.0001 ‡ Multivariate \* 34.3 ± 9.9 0.0007 ‡ 64.3 ± 10.1 <0.0001 ‡ BMI 4.1 ± 0.7 <0.0001 ‡ 4.4 ± 0.7 <0.0001 ‡ Multivariate \* 4.2 ± 0.6 <0.0001 ‡ 4.4 ± 0.7 <0.0001 ‡ Ever-smoker 15.2 ± 8.7 0.08 15.9 ± 9.2 0.08 Multivariate \* 14.3 ± 8.4 0.09 15.2 ± 9.06 0.09 ILD 22.6 ± 8.9 0.01 ‡ 18.3 ± 9.1 0.05 ‡ Multivariate † 4.6 ± 7.8 0.55 ‡ −0.3 ± 7.0 0.96 Diabetes 60.1 ± 21.7 0.0063 35.9 ± 23.5 0.13 Multivariate † 38.2 ± 18.5 0.04 ‡ 12.6 ± 18.0 0.48 Hyperlipidemia 24.6 ± 10.2 0.02 ‡ 41.9 ± 10.5 <0.0001 ‡ Multivariate † -2.5 ± 9.3 0.78 10.03 ± 8.9 0.26 CAC 27.1 ± 8.7 0.0020 ‡ 32.11 ± 9.2 0.0006 Multivariate † 9.4 ± 8.5 0.27 8.7 ± 8.15 0.29
BMI, body mass index; CAC, coronary artery calcium; ILD, interstitial lung disease; SE, standard error.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
ITFV and Presence of SSc
Get Radiology Tree app to read full this article<
![Figure 3, Column graph showing intrathoracic fat volumes and body mass index (BMI) in controls and systemic sclerosis (SSc) patients without and with associated pulmonary arterial hypertension (PAH). Intrathoracic fat volumes (epicardial fat volume [EFV], extrapericardial fat volume [EPFV], and intrathoracic fat volume [ITFV] are scaled to the left y-axis, and BMI is scaled to the right y-axis). This graph demonstrates significant difference of epicardial fat volume across the groups, whereas BMI demonstrates no difference across the groups. Note that patients with SSc-associated PAH have the most extensive epicardial fat volume than patients with SSc alone and controls.](https://storage.googleapis.com/dl.dentistrykey.com/clinical/IncreasedEpicardialFatVolumeIsIndependentlyAssociatedwiththePresenceandSeverityofSystemicSclerosis/2_1s20S1076633217303276.jpg)
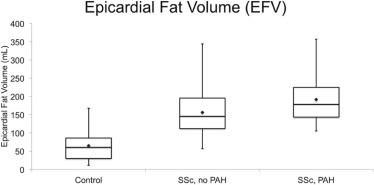
TABLE 3
(a) Logistic Regression Analysis for Systemic Sclerosis Versus Control and (b) Logistic Regression Analysis for Systemic Sclerosis Versus Systemic Sclerosis-Associated Pulmonary Arterial Hypertension
(a) Systemic Sclerosis Versus Controls OR (95% CI)P Value EFV Unadjusted 1.058 (1.042–1.075) <0.0001 Adjusted \* 1.065 (1.046–1.084) <0.0001 EPFV \* Unadjusted 1.014 (1.007–1.021) 0.0001 Adjusted \* 1.028 (1.017–1.038) <0.0001 ITFV \* Unadjusted 1.022 (1.016–1.028) <0.0001 Adjusted \* 1.033 (1.023–1.043) <0.0001
(b) SSc without PAH Versus SSc with PAH OR (95% CI)P Value EFV Unadjusted 1.010 (1.004–1.015) 0.0002 Model 1 1.008 (1.001–1.015) 0.025 Model 2 1.008 (1.000–1.015) 0.044 EPFV Unadjusted 1.006 (1.002–1.011) 0.009 Model 1 1.002 (0.995–1.009) 0.52 Model 2 0.998 (0.991–1.006) 0.70 ITFV Unadjusted 1.005 (1.002–1.008) 0.0004 Model 1 1.004 (1.000–1.008) 0.083 Model 2 1.002 (0.998–1.007) 0.304 CAC Unadjusted 4.529 (2.228–9.208) < 0.0001 Model 1 1.826 (0.782–4.267) 0.1642 Model 2 2.184 (0.878–5.432) 0.09
CAC, coronary artery calcium; CI, confidence interval; EFV, epicardial fat volume; EPFV, extrapericardial fat volume; ITFV, intrathoracic fat volume; OR, odds ratio; PAH, pulmonary arterial hypertension; SSc, systemic sclerosis.
Models 1: adjusted for age, gender, body mass index, hyperlipidemia, smoking, CAC, and diabetes. Model 2: adjusted for age, gender, body mass index, hyperlipidemia, smoking, diabetes, CAC, and interstitial lung disease.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
ITFV and Severity of SSc (PAH Versus No PAH)
Get Radiology Tree app to read full this article<
Discussion
Main Results
Get Radiology Tree app to read full this article<
ITFV and Presence of SSc
Get Radiology Tree app to read full this article<
ITFV and Severity of SSc (SSc-PAH)
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Prior Studies
Get Radiology Tree app to read full this article<
Limitations
Get Radiology Tree app to read full this article<
Conclusion
Get Radiology Tree app to read full this article<
Acknowledgements
Get Radiology Tree app to read full this article<
References
1. Barnes J., Mayes M.D.: Epidemiology of systemic sclerosis. Curr Opin Rheumatol 2012; 24: pp. 165-170.
2. Lambova S.: Cardiac manifestations in systemic sclerosis. World J Cardiol 2014; 6: pp. 993-1005.
3. Elhai M., Avouac J., Kahan A., et. al.: Systemic sclerosis: recent insights. Joint Bone Spine 2015; 82: pp. 148-153.
4. Leduc C., Young I.D., Joneja M.G., et. al.: Unexpected post-mortem diagnosis of systemic sclerosis presenting as pneumatosis intestinalis: revised diagnostic criteria and medicolegal implications. Leg Med (Tokyo) 2015; 17: pp. 29-33.
5. Torres T., Bettencourt N., Mendonça D., et. al.: Epicardial adipose tissue and coronary artery calcification in psoriasis patients. J Eur Acad Dermatol Venereol 2015; 29: pp. 270-277.
6. Lima-Martinez M.M., Campo E., Salazar J., et. al.: Epicardial fat thickness as cardiovascular risk factor and therapeutic target in patients with rheumatoid arthritis treated with biological and nonbiological therapies. Arthritis 2014; 2014: pp. 782850.
7. Noyes A.M., Dua K., Devadoss R., et. al.: Cardiac adipose tissue and its relationship to diabetes mellitus and cardiovascular disease. World J Diabetes 2014; 5: pp. 868-876.
8. Okada K., Ohshima S., Isobe S., et. al.: Epicardial fat volume correlates with severity of coronary artery disease in nonobese patients. J Cardiovasc Med (Hagerstown) 2014; 15: pp. 384-390.
9. Katsiki N., Mikhailidis D.P., Wierzbicki A.S.: Epicardial fat and vascular risk: a narrative review. Curr Opin Cardiol 2013; 28: pp. 458-463.
10. Dozio E., Briganti S., Vianello E., et. al.: Epicardial adipose tissue inflammation is related to vitamin D deficiency in patients affected by coronary artery disease. Nutr Metab Cardiovasc Dis 2015; 25: pp. 267-273.
11. Mazurek T.: Human epicardial adipose tissue is a source of inflammatory mediators. Circulation 2003; 108: pp. 2460-2466.
12. Yorgun H., Canpolat U., Aytemir K., et. al.: Association of epicardial and peri-atrial adiposity with the presence and severity of non-valvular atrial fibrillation. Int J Cardiovasc Imaging 2015; 31: pp. 649-657.
13. Stojanovska J., Kazerooni E.A., Sinno M., et. al.: Increased epicardial fat is independently associated with the presence and chronicity of atrial fibrillation and radiofrequency ablation outcome. Eur Radiol 2015; 25: pp. 2298-2309.
14. Sacks H.S., Fain J.N.: Human epicardial adipose tissue: a review. Am Heart J 2007; 153: pp. 907-917.
15. Harada K., Amano T., Kataoka T., et. al.: Impact of abdominal and epicardial fat on the association between plasma adipocytokine levels and coronary atherosclerosis in non-obese patients. Atherosclerosis 2014; 237: pp. 671-676.
16. Baysal E., Yilmaz N., Karadag O., et. al.: Epicardial adipose tissue thickness and systemic sclerosis. Acta Medica Maditerranea 2015; 31: pp. 97-101.
17. Spearman J.V., Renker M., Schoepf U.J., et. al.: Prognostic value of epicardial fat volume measurements by computed tomography: a systematic review of the literature. Eur Radiol 2015; 25: pp. 3372-3381.
18. Bucher A.M., Schoepf U.J., Krazinski A.W., et. al.: Influence of technical parameters on epicardial fat volume quantification at cardiac CT. Eur J Radiol 2015; 84: pp. 1062-1067.
19. Chaisson N.F., Hassoun P.M.: Systemic sclerosis-associated pulmonary arterial hypertension. CHEST J 2013; 144: pp. 1346.
20. Fischer A., Swigris J.J., Bolster M.B., et. al.: Pulmonary hypertension and interstitial lung disease within PHAROS: impact of extent of fibrosis and pulmonary physiology on cardiac haemodynamic parameters. Clin Exp Rheumatol 2014; 32: pp. S109-S114.
21. Thakkar V., Nikpour M., Stevens W.M., et. al.: Prospects for improving outcomes in systemic sclerosis-related pulmonary hypertension. Intern Med J 2015; 45: pp. 248-254.
22. Kiani A.N., Magder L.S., Post W.S., et. al.: Coronary calcification in SLE: comparison with the Multi-Ethnic Study of Atherosclerosis. Rheumatology 2015; 54: pp. 1976-1981.
23. Khurma V., Meyer C., Park G.S., et. al.: A pilot study of subclinical coronary atherosclerosis in systemic sclerosis: coronary artery calcification in cases and controls. Arthritis Care Res 2008; 59: pp. 591-597.
24. Mok M.Y., Lau C.S., Sau S., et. al.: Systemic sclerosis is an independent risk factor for increased coronary artery calcium deposition. Arthritis Rheum 2011; 63: pp. 1387-1395.
25. Hoogen F., Van Den Khanna D., Fransen J., et. al.: Arthritis & rheumatism 2013 classification criteria for systemic sclerosis.2013. 65:2737–2747
26. Egan B.M., Zhao Y., Axon R.N.: US trends in prevalence, awareness, treatment and Control of Hypertension, 1988–2008. JAMA 2010; 303: pp. 2043-2050.
27. NCEP : Executive summary of the third report of the national cholesterol education program expert panel on detection, evaluation and treatment of high blood cholesterol in adults (Adult Treatment Panel III). JAMA 2001; 285: pp. 2486-2497.
28. Mahabadi A.A., Massaro J.M., Rosito G.A., et. al.: Association of pericardial fat, intrathoracic fat, and visceral abdominal fat with cardiovascular disease burden: the Framingham Heart Study. Eur Heart J 2009; 30: pp. 850-856.
29. Galiè N., Humbert M., Vachiery J.-L., et. al.: 2015 ESC/ERS Guidelines for the diagnosis and treatment of pulmonary hypertension. Eur Heart J 2015; 37: pp. 67-119.
30. Coghlan J.G., Denton C.P., Grünig E., et. al.: Evidence-based detection of pulmonary arterial hypertension in systemic sclerosis: the DETECT study. Ann Rheum Dis 2014; 73: pp. 1340-1349.
31. Visovatti S.H., Distler O., Coghlan J.G., et. al.: Borderline pulmonary arterial pressure in systemic sclerosis patients: a post-hoc analysis of the DETECT study. Arthritis Res Ther 2014; 16: pp. 493.
32. Stojanovska J., Ibrahim E., Chughtai A.R., et. al.: Intra-thoracic fat measurements using multidetector computed tomography (MDCT): feasibility and reproducibility. Tomography 2017; 3: pp. 33-40.
33. Borkan G.A., Gerzof S.G., Robbins A.H., et. al.: Assessment of abdominal fat content by computed tomography. Am J Clin Nutr 1982; 36: pp. 172-177.
34. Kim Y.K., Sung Y.M., Cho S.H., et. al.: Reliability analysis of visual ranking of coronary artery calcification on low-dose CT of the thorax for lung cancer screening: comparison with ECG-gated calcium scoring CT. Int J Cardiovasc Imaging 2014; 30: pp. 81-87.
35. Ormseth M.J., Lipson A., Alexopoulos N., et. al.: Epicardial adipose tissue is associated with cardiometabolic risk and the metabolic syndrome in patients with rheumatoid arthritis. Arthritis Care Res 2013; 65: pp. 1410-1415.
36. Fuschiotti P.: Current perspectives on the immunopathogenesis of systemic sclerosis. Immunotargets and Therapy. Immunotargets 2016; 5: pp. 21-35.
37. McLaughlin V.V., Shah S.J., Souza R., et. al.: Management of pulmonary arterial hypertension. J Am Coll Cardiol 2015; 65: pp. 1976-1997.
38. Simonneau G., Galie N., Rubin L.J., et. al.: Clinical classification of pulmonary hypertension. J Am Coll Cardiol 2004; 43: pp. 5S-12S.
39. Lambova S., Müller-Ladner U.: Pulmonary arterial hypertension in systemic sclerosis. Autoimmun Rev 2010; 9: pp. 761-770.
40. Iacobellis G., Corradi D., Sharma A.M.: Epicardial adipose tissue: anatomic, biomolecular and clinical relationships with the heart. Nat Clin Pract Cardiovasc Med 2005; 2: pp. 536-543.
41. Dabbah S., Komarov H., Marmor A., et. al.: Nutrition, metabolism & cardiovascular diseases epicardial fat, rather than pericardial fat is independently associated with diastolic filling in subjects without apparent heart disease. Nutr Metab Cardiovasc Dis 2014; 24: pp. 877-882.
42. Hatem N., Redheuil A., Gandjbakhch E.: Cardiac adipose tissue and atrial fibrillation: the perils of adiposity. Cardiovasc Res 2016; 109: pp. 502-509.
43. Cavalcante J.L., Tamarappoo B.K., Hachamovich R., et. al.: Association of epicardial fat, hypertension, subclinica; coronary artery disease, and metabolic syndrome with left ventricular diastolic dysfunction. Am J Cardiol 2012; 110: pp. 1793-1798.