
Rationale and Objectives
To assess computed tomographic (CT) signs that have been described in published studies for the diagnosis of appendicitis to identify independent findings that predict appendicitis.
Methods and Materials
A retrospective database search identified 67 patients with a CT scan of the abdomen/pelvis and pathologic evaluation of the appendix, including 41 with appendicitis and 26 with a normal appendix on pathologic examination. Each computed tomogram was re-evaluated by three independent, blinded observers who evaluated appendix diameter, enhancement of the appendix, thickening of the appendix, presence of an appendicolith, infiltration of peri-appendiceal fat, focal cecal thickening, local lymphadenopathy, fluid collections, non-appendiceal bowel thickening, non-periappendiceal infiltration of fat, and comparison of peri-appendiceal fat infiltration to thickening of adjacent bowel loops.
Results
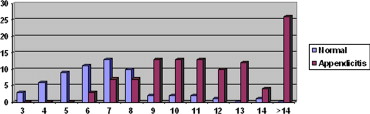
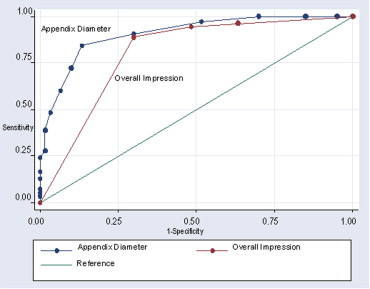
Mean diameter of the normal appendix (6.7 ± 2.2 mm) was significantly lower than that of the inflamed appendix (12.1 ± 4.3 mm; P < .001). Significant univariate predictors of appendicitis included appendix diameter >8 mm (odds ratio [OR] 34.8), enhancement of the appendix (OR 4.4), thickening of the appendix (OR 4.3), infiltration of peri-appendiceal fat (OR 5.5), focal cecal thickening (OR 5.1), non-appendiceal bowel thickening (OR 0.4), and non-periappendiceal infiltration of fat (OR = 0.3). Of these variables, only appendix diameter and enhancement of the appendix were significant independent predictors of appendicitis on multivariate analysis. An overall diagnostic impression based on all secondary signs was less accurate than a diagnosis based on appendix diameter alone (receiver-operating characteristic analysis: Az = 0.80 vs. Az = 0.91, P = .02). Sensitivity/specificity of appendix diameter was 84%/87% using a cutoff between 8 and 9 mm and 97%/48% using a cutoff between 6 and 7 mm.
Conclusion
Appendix diameter is the best single diagnostic criterion for appendicitis on CT scan. A cutoff between 8 and 9 mm provided the best balance of sensitivity/specificity in our study population, whereas a cutoff between 6 and 7 mm improved sensitivity at the expense of specificity. The presence of appendiceal enhancement provided additional diagnostic information, but other secondary signs of appendicitis did not improve diagnostic accuracy.
Appendicitis is the most commonly encountered cause of abdominal pain requiring surgical management ( ). Delayed or inaccurate diagnosis of appendicitis can lead to significant morbidity and mortality. Within the United States, there are a reported one million hospital days per year from 250,000 cases annually of appendicitis ( ). The incidence of appendicitis is greatest in the second decade of life ( ).
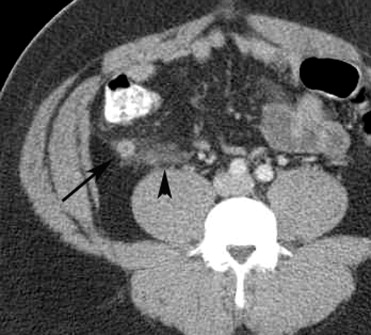
Computed tomography has been advocated as a cost-efficient and accurate way to diagnose appendicitis, particularly in the setting of an inconclusive clinical examination ( ). In many hospitals, computed tomography is considered the standard of care for the evaluation of suspected appendicitis (7). Computed tomographic (CT) findings described in published studies that suggest a diagnosis of appendicitis include the presence of an enlarged appendix measuring larger than 6 mm in diameter, appendiceal wall thickening, peri-appendiceal fat stranding, the presence of an appendicolith, and appendiceal wall enhancement ( ). Other CT signs of appendicitis are adjacent bowel wall thickening, cecal apical thickening, the “cecal bar” or arrowhead sign, adjacent fat stranding, the presence of an abscess, and lymphadenopathy ( ). In 13% of cases performed for the evaluation of acute appendicitis, the appendix is not visualized, and secondary findings related to appendicitis are used for the diagnosis ( ).
Get Radiology Tree app to read full this article<
Materials and methods
Database Search
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
CT Scan Protocol
Get Radiology Tree app to read full this article<
Scan Interpretation
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 1
Study Form Completed for Each Subject
•Appendix visualized Y N •Appendix diameter (outer to outer wall) ______ mm •Appendicolith Y N •Appendiceal wall enhancement Y N •Appendiceal wall thickening Y N •Peri-appendiceal fat stranding None mild moderate severe •Fat stranding not at appendix Y N •Non-appendiceal bowel wall thickening Y N •Fat stranding: bowel wall thickening None/equal/mildly greater/moderately greater/markedly greater •Focal cecal apical thickening Y N •Right lower quadrant lymphadenopathy None Normal size Enlarged •Peri-appendiceal or adjacent abscess Y N •Overall suspicion for appendicitis None/probably not/probably is/definite
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Univariate analysis
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Multivariate analysis
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Receiver-operating characteristic analysis
Get Radiology Tree app to read full this article<
Interobserver Agreement
Get Radiology Tree app to read full this article<
Results
Study Population Demographics
Get Radiology Tree app to read full this article<
Pathology
Get Radiology Tree app to read full this article<
Visualization of Appendix
Get Radiology Tree app to read full this article<
Univariate Analysis
Get Radiology Tree app to read full this article<


Get Radiology Tree app to read full this article<
Multivariate Analysis
Get Radiology Tree app to read full this article<
Appendix Diameter
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Overall Impression
Get Radiology Tree app to read full this article<
Table 2
Univariate Analysis
Observation #1 #2 #3 Overall OR_P_ Value AP diameter 49.5 53.2 18.8 34.8 <.001 AP stone 0.82 10.0 2.7 1.1 .81 AP enhancement 6.9 2.7 5.2 4.4 .001 Arrow sign 4.0 1.3 17 5.1 .002 AP wall thickening 6.7 4.3 3.1 4.3 <.001 Peri-AP stranding 4.4 9.7 3.7 5.5 .001 Other fat stranding 0.34 0.13 0.28 0.30 .008 Other wall thickening 0.41 0.56 0.28 0.40 .07 Peri-AP stranding vs. other wall thickening (5 patients) 0.65 1.41 1.58 1.2 .36 Lymphadenopathy (3 patients) 0.95 1.27 2.02 1.2 .44 Abscess 0.88 0.40 0.31 0.57 .35 Overall impression 18.0 14.1 31.5 18.2 <.001 AP, anteroposterior; OR, odds ratio.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Cases with Diameter <9 mm
Get Radiology Tree app to read full this article<
Cases with Nonvisualized Appendix
Get Radiology Tree app to read full this article<
Interobserver Agreement
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Macari M., Balthazar E.J.: The acute right lower quadrant: CT evaluation. Radiol Clin N Am 2003; 41: pp. 1117-1136.
2. Addiss D.G., Shaffer N., Fowler B.S., et. al.: The epidemiology of appendicitis and appendectomy in the United States. Am J Epidemiol 1990; 132: pp. 910-925.
3. Birnbaum B.A., Wilson S.R.: Appendicitis at the millennium. Radiology 2000; 215: pp. 337-348.
4. Rao P.M., Rhea J.T., Novelline R.A.: Helical CT of appendicitis and diverticulitis. Radiol Clin N Am 1999; 41: pp. 895-902.
5. Rao P.M., Rhea J.T., Novelline R.A., et. al.: Effect of computed tomography of the appendix on treatment of patients and use of hospital resources. N Engl J Med 1998; 338: pp. 141-146.
6. Hansen A.J., Young S.W., De Petris G., et. al.: Histologic severity of appendicitis can be predicted by computed tomography. Arch Surg 2004; 139: pp. 1304-1308.
7. Raptopoulos V., Katsou G., Rosen M.P., et. al.: Acute appendicitis: effect of increased use of CT on selecting patients earlier. Radiology 2003; 226: pp. 521-526.
8. Paulson E.K., Kalady M.F., Pappas T.N.: Suspected appendicitis. N Engl J Med 2003; 348: pp. 236-242.
9. Choi D., Park H., Lee Y.R., et. al.: Most useful findings for diagnosing acute appendicitis on contrast-enhanced helical CT. Acta Radiol 2003; 44: pp. 574-582.
10. Rettenbacher T., Hollerweger A., Macheiner P., et. al.: Outer diameter of the vermiform appendix as a sign of acute appendicitis: evaluation at US. Radiology 2001; 218: pp. 757-762.
11. Keyzer C., Tack D., Maertelaer V.: Acute appendicitis: comparison of low-dose and standard-dose unenhanced multi-detector row CT. Radiology 2004; 232: pp. 164-172.
12. Pereira J., Sirlin C., Pinto P.: Disproportionate fat stranding: a helpful CT sign in patients with acute abdominal pain. Radiographics 2004; 24: pp. 703-715.
13. Neumayer L., Kennedy A.: Imaging in appendicitis: a review with special emphasis on the treatment of women. Obstet Gynecol 2003; 102: pp. 1404-1409.
14. Balthazar E.J., Megibow A.J., Gordon R.B., et. al.: Computed tomography of the abnormal appendix. J Comput Assist Tomogr 1988; 12: pp. 595-601.
15. Rao P.M., Rhea J.T., Novelline R.A.: Sensitivity and specificity of the individual CT signs of appendicitis: experience with 200 helical appendiceal CT examinations. J Comput Assist Tomogr 1997; 21: pp. 686-692.
16. Rexroad J.T.: The CT arrowhead sign. Radiology 2003; 227: pp. 44-45.
17. Checkoff J.L., Wechsler R.J., Nazarian L.N.: Chronic inflammatory appendiceal conditions that mimic acute appendicitis on helical CT. AJR Am J Roentgenol 2002; 179: pp. 731-734.
18. Kalidon E., Pikoulis E., Katsiva V., et. al.: Spiral computed tomography: a diagnostic aid in patients with atypical appendicitis. Acta Chirugica Belgia 2006; 106: pp. 47-51.
19. Nikolaidis P., Hwang C.M., Miller F.M., et. al.: Nonvisualized appendix: incidence of acute appendicitis when secondary inflammatory changes are absent. AJR Am J Roentgenol 2004; 183: pp. 889-892.
20. Raman S.S., Lu D.S., Kadell B.M., et. al.: Accuracy of nonfocused Helical CT for the diagnosis of acute appendicitis: a 5-year review. AJR Am J Roentgenol 2002; 178: pp. 1319-1325.
21. Mittal V.K., Goliath J., Sabir M.: Advantages of focused helical computed tomographic scanning with rectal contrast only vs. triple contrast in the diagnosis of clinically uncertain acute appendicitis: a prospective randomized study. Arch Surg 2004; 139: pp. 495-499.
22. Balthazar E.J., Rofsky N.M., Zucker R.: Appendicitis: the impact of computed tomography imaging on negative appendectomy and perforation rates. Am J Gastroenterol 1998; 93: pp. 768-771.
23. Balthazar E.J., Birnbaum B.A., Yee J., et. al.: Acute appendicitis: CT and US correlation in 100 patients. Radiology 1994; 190: pp. 31-35.
24. Quillin S.P., Siegel M.J.: Appendicitis: efficacy of color Doppler sonography. Radiology 1994; 191: pp. 557-560.
25. Johnson P.T., Eng J., Moore C.J., et. al.: Multidetector-row CT of the appendix in healthy adults. Emerg Radiol 2006; 12: pp. 248-253.
26. Tamburrini S., Brunetti A., Brown M., et. al.: CT appearance of the normal appendix in adults. Eur Radiol 2005; 15: pp. 2096-2103.
27. Cobben L.P., Otterloo A.M., Puylaert J.B.: Spontaneously resolving appendicitis: frequency and natural history in 60 patients. Radiology 2000; 215: pp. 349-352.
28. Daly C.P., Cohan R.H., Francis I.R., et. al.: Incidence of acute appendicitis in patients with equivocal CT findings. AJR Am J Roentgenol 2005; 184: pp. 1813-1820.