
Rationale and Objectives
Although inflammatory breast carcinoma (IBC) accounts for 1%–4% of all breast cancer cases, the appearance of this highly malignant tumor in magnetic resonance imaging (MRI) is still not well characterized. The aim of this study was to identify typical imaging features of IBC in comparison with noninflammatory locally advanced breast carcinoma (LABC).
Materials and Methods
MRIs of 48 patients with IBC were compared with an equivalent cohort of 52 subjects with LABC. Age and histopathologic subtype were equivalent between the two groups. To delineate characteristic features, a multitude of dynamic and morphologic parameters were evaluated using T1- and T2-weighted sequences.
Results
No significant differences of prevalences could be found for the following criteria: dynamic tumor signal characteristics, prominent vessels, perifocal edema, axillary lymph node involvement, morphology of focal masses, and morphologic pattern of non–mass like enhancement. Otherwise, the quantity of focal masses and the spatial distribution of the tumoral infiltration significantly differed between the two cancer groups. The following parameters occurred more frequently in the IBC cases: edema (cutaneous/subcutaneous 81.3%, perimamillar 70.8%, diffuse 89.6%, prepectoral 72.9%, intramuscular pectoral 41.7%), thickening (75.0%) and pathologic enhancement (60.4%) of Cooper’s ligaments, skin thickening (83.3%), punched-out sign (initially strong, focal increase of some dermal or subcutaneous parts followed by slow-continuous enhancement of the surrounding skin; 56.3%).
Conclusions
Inflammatory breast carcinoma seems to represent a specific biological entity resulting in typical MRI characteristics. Some of the parameters are supposed to visualize the characteristic extensive lymphovascular infiltration and therefore may improve the diagnosis of IBC.
Inflammatory breast carcinoma (IBC) is a very malignant form of invasive breast cancer with a tendency to metastasize at an early stage, resulting in a poor outcome ( ). This aggressive variant accounts for about 1%–4% of all breast cancer cases with an increasing incidence rate, probably because of changing patterns of risk factor exposure ( ). The term inflammatory carcinoma derives from the inflammatory-like symptoms that are associated with this cancer type; typical clinical manifestations are increased volume and induration of the breast, pain, peau d’orange appearance, increased cutaneous temperature, dermal redness of at least one-third of the breast, and the presence of a palpable mass ( ).
The clinical manifestations of IBC are histologically related to dermal or subcutaneous lymphatic infiltration by tumor emboli that obstruct the lymphatic capillaries ( ). However, lymphatic infiltration of the skin cannot be detected by histology in all patients suffering from IBC. Thus, inflammatory breast carcinoma comprises the following subtypes ( ): the presence of both clinical symptoms of inflammation and dermal or subcutaneous lymphatic tumoral invasion verified by histology, accounts for about 50% and is known as common IBC . A further 40% is only characterized by the appearance of clinical signs in the absence of histopathologically verified lymphatic infiltration and is consecutively named clinical IBC . A small proportion of cases, about 10%, do not present any clinical inflammatory signs, and the diagnosis is only made by lymphatic invasion of the skin, the so-called occult IBC . This occult inflammatory carcinoma is proved to show a better prognosis than the other two types and may therefore be an early IBC form ( ).
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
 Open full size image
Open full size image
Figure 1
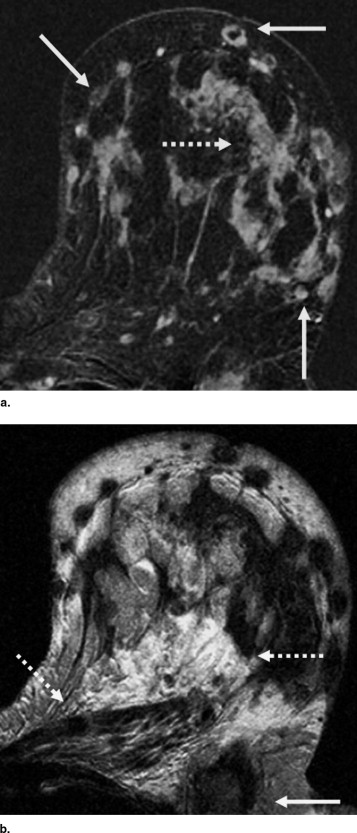
A 43-year-old woman with inflammatory carcinoma (invasive lobular, G3) in the left breast. The craniocaudal (a) and mediolateral-oblique (b) mammogram demonstrates a diffuse increase of breast density and skin thickening. The magnetic resonance examination ( c: subtraction 1 minute after bolus injection; d: T2-weighted image) shows the tumor characteristics in much more detail: the diffuse enhancement infiltrating the skin and the pectoralis muscle (continuous arrows), and edema in a cutaneous/subcutaneous, diffuse, and prepectoral localization (discontinuous arrows).
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Materials and methods
Subjects
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
MR Mammography
Get Radiology Tree app to read full this article<
Evaluation Criteria
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results
Patient Characteristics
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Histopathologic Results
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Dynamic Criteria
Get Radiology Tree app to read full this article<
Table 1
Signal Kinetic Characteristics of Inflammatory Carcinomas and Locally Advanced Cancers
Inflammatory Breast Carcinomas ( n = 48) Locally Advanced Cancers ( n = 52)P Values of Pearson’s Chi-Square Test (Two-Sided) Initial signal increase <50% 1 (2.1) 1 (1.9) 50%–100% 6 (12.5) 10 (19.2) >.05 >100% 41 (85.4) 41 (78.9) Postinitial enhancement Continuous increase 4 (8.3) 3 (5.8) Plateau phenomenon 11 (22.9) 15 (28.8) >.05 Washout sign 33 (68.8) 34 (65.4)
Numbers in parentheses are percentages.
Get Radiology Tree app to read full this article<
Analysis of Focal Masses
Get Radiology Tree app to read full this article<
Table 2
Analysis of Focal Masses of Inflammatory Carcinomas and Locally Advanced Cancers
Inflammatory Breast Carcinomas ( n = 40) Locally Advanced Cancers ( n = 52)P Values of Pearson’s Chi-Square Test (Two-Sided) Quantity 1 focal mass 4 (10.0) 24 (46.2) <.001 2–4 masses 13 (32.5) 18 (34.6) 5–7 masses 7 (17.5) 5 (9.6) >7 masses 16 (40.0) 5 (9.6) Shape Round 15 (37.5) 21 (40.4) >.05 Oval 8 (20.0) 9 (17.3) Lobulated 5 (12.5) 4 (7.7) Irregular 12 (30.0) 18 (34.6) Margin Smooth 7 (17.5) 5 (9.6) >.05 Irregular 23 (57.5) 36 (69.2) Spiculated 10 (25.0) 11 (21.2)
Numbers in parentheses are percentages.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Evaluation of Tumoral Infiltration
Get Radiology Tree app to read full this article<
Table 3
Analysis of Non–Mass-Like Enhancement of Inflammatory Carcinomas and Locally Advanced Cancers
Inflammatory Breast Carcinomas ( n = 48) Locally Advanced Cancers ( n = 26)P Values of Pearson’s Chi-Square Test (Two-Sided) Spatial distribution Linear/ductal 0 (0.0) 2 (7.7) <.001 Segmental 7 (14.6) 13 (50.0) Regional 9 (18.7) 5 (19.2) Multiple regions 11 (22.9) 5 (19.2) Diffuse 21 (43.8) 1 (3.9) Internal enhancement Stippled/punctate 14 (29.2) 7 (26.9) >.05 Clumped 11 (22.9) 5 (19.2) Dendritic 17 (35.4) 10 (38.5) Nonspecific 6 (12.5) 4 (15.4)
Numbers in parentheses are percentages.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 4
Evaluation of Morphologic Parameters of the Breast of Inflammatory Carcinomas and Locally Advanced Cancers
Inflammatory Breast Carcinomas ( n = 48) Locally Advanced Cancers ( n = 52)P Values of Fisher’s Exact Test (Two-Sided) Edema subtypes Cutaneous/subcutaneous 39 (81.3) 15 (28.8) <.001 Perimamillar 34 (70.8) 13 (25.0) <.001 Perifocal 32 (66.7) 37 (71.2) >.05 Diffuse 43 (89.6) 19 (36.5) <.001 Prepectoral 35 (72.9) 20 (38.5) <.01 Intramuscular pectoral 20 (41.7) 8 (15.4) <.01 Cooper’s ligaments Trabecular thickening 36 (75.0) 17 (32.7) <.001 Enhancing ligaments 29 (60.4) 13 (25.0) <.01 Skin involvement Diffuse skin thickening 40 (83.3) 15 (28.8) <.001 Punched-out sign 27 (56.3) 5 (9.6) <.001 Prominent vessels 41 (85.4) 40 (76.9) >.05 Lymph node involvement 32 (66.7) 28 (53.8) >.05
Numbers in parentheses are percentages.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<

Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Jaiyesimi I.A., Buzdar A.U., Hortobagyi G.: Inflammatory breast cancer: a review. J Clin Oncol 1992; 10: pp. 1014-1024.
2. Hance K.W., Anderson W.F., Devesa S.S., et. al.: Trends in inflammatory breast carcinoma incidence and survival: the surveillance, epidemiology, and end results program at the National Cancer Institute. J Natl Cancer Inst 2005; 97: pp. 966-975.
3. Rosen P.P.: Inflammatory carcinoma.Rosen P.P.Rosen’s breast pathology.2001.Lippincott Williams & WilkinsPhiladelphia, PA:pp. 676-687.
4. Amparo R.S., Angel C.D., Ana L.H., et. al.: Inflammatory breast carcinoma: pathological or clinical entity?. Breast Cancer Res Treat 2000; 64: pp. 269-273.
5. Wilke D., Colwell B., Dewar R.: Inflammatory breast carcinoma: comparison of survival of those diagnosed clinically, pathologically, or with both features. Am Surg 1998; 64: pp. 428-431.
6. Lee K.W., Chung S.Y., Yang I., et. al.: Inflammatory breast cancer: imaging findings. Clin Imaging 2005; 29: pp. 22-25.
7. Belli P., Costantini M., Romani M., et. al.: Role of magnetic resonance imaging in inflammatory carcinoma of the breast. Rays 2002; 27: pp. 299-305.
8. Günhan-Bilgen I., Üstün E.E., Memis A.: Inflammatory breast carcinoma: mammographic, ultrasonographic, clinical, and pathologic findings in 142 cases. Radiology 2002; 223: pp. 829-838.
9. Kushwaha A.C., Whitman G.J., Stelling C.B., et. al.: Primary inflammatory carcinoma of the breast: retrospective review of mammographic findings. AJR Am J Roentgenol 2000; 174: pp. 535-538.
10. Orel S.G., Schnall M.D.: MR imaging of the breast for the detection, diagnosis, and staging of breast cancer. Radiology 2001; 220: pp. 13-30.
11. Kuhl C.K.: Current status of breast MR imaging: part 2. Clinical applications. Radiology 2007; 244: pp. 672-691.
12. Chou C.P., Wu M.T., Chang H.T., et. al.: Monitoring breast cancer response to neoadjuvant systemic chemotherapy using parametric contrast-enhanced MRI: a pilot study. Acad Radiol 2007; 14: pp. 561-573.
13. Berg W.A., Gutierrez L., NessAiver M.S., et. al.: Diagnostic accuracy of mammography, clinical examination, US, and MR imaging in preoperative assessment of breast cancer. Radiology 2004; 233: pp. 830-849.
14. Friedman P., Sanders L., Russo J., et. al.: Detection and localization of occult lesions using breast magnetic resonance imaging: initial experience in a community hospital. Acad Radiol 2005; 12: pp. 728-738.
15. Kaiser W.A., Zeitler E.: MR imaging of the breast: fast imaging sequences with and without Gd-DTPA. Radiology 1989; 170: pp. 681-686.
16. Heywang-Köbrunner S.H., Viehweg P., Heinig A., et. al.: Contrast-enhanced MRI of the breast: accuracy, value, controversies, solutions. Eur J Radiol 1997; 24: pp. 94-108.
17. Kuhl C.K., Mielcareck P., Klaschik S., et. al.: Dynamic breast MR imaging: are signal intensity time course data useful for differential diagnosis of enhancing lesions?. Radiology 1999; 211: pp. 101-110.
18. Sherif H., Mahfouz A.E., Oellinger H., et. al.: Peripheral washout sign on contrast-enhanced MR images of the breast. Radiology 1997; 205: pp. 209-213.
19. Daniel B.L., Yen Y.F., Glover G.H., et. al.: Breast disease: dynamic spiral MR imaging. Radiology 1998; 209: pp. 499-509.
20. Mussurakis S., Buckley D.L., Drew P.J., et. al.: Dynamic MR imaging of the breast combined with analysis of contrast agent kinetics in the differentiation of primary breast tumours. Clin Radiol 1997; 52: pp. 516-526.
21. Baum F., Fischer U., Vosshenrich R., et. al.: Classification of hypervascularized lesions in CE MR imaging of the breast. Eur Radiol 2002; 12: pp. 1087-1092.
22. Chen W., Giger M.L., Bick U.: A fuzzy c-means (FCM)-based approach for computerized segmentation of breast lesions in dynamic contrast-enhanced MR images. Acad Radiol 2006; 13: pp. 63-72.
23. Kuhl C.K., Klaschik S., Mielcarek P., et. al.: Do T2-weighted pulse sequences help with the differential diagnosis of enhancing lesions in dynamic breast MRI?. J Magn Reson Imaging 1999; 9: pp. 187-196.
24. Fischer D.R., Wurdinger S., Böttcher J., et. al.: Further signs in the evaluation of magnetic resonance mammography: a retrospective study. Invest Radiol 2005; 40: pp. 430-435.
25. Malich A., Fischer D.R., Wurdinger S., et. al.: Potential MRI interpretation model: differentiation of benign from malignant breast masses. AJR Am Roentgenol 2005; 185: pp. 964-970.
26. Rieber A., Tomczak R.J., Mergo P.J., et. al.: MRI of the breast in the differential diagnosis of mastitis versus inflammatory carcinoma and follow-up. J Comput Assist Tomogr 1997; 21: pp. 128-132.
27. Tomczak R.J., Rieber A., Zeitler H., et. al.: The value of MR-mammography at 1.5 tesla in the differential diagnosis of non-puerperal mastitis and inflammatory breast carcinoma. Rofo 1996; 165: pp. 148-151.
28. Yasumura K., Ogawa K., Ishikawa H., et. al.: Inflammatory carcinoma of the breast: characteristic findings of MR imaging. Breast Cancer 1997; 4: pp. 161-169.
29. Anderson W.F., Chu K.C., Chang S.: Inflammatory breast carcinoma and noninflammatory locally advanced breast carcinoma: distinct clinicopathologic entities?. J Clin Oncol 2003; 21: pp. 2254-2259.
30. Lerebours F., Bieche I., Lidereau R.: Update on inflammatory breast cancer. Breast Cancer Res 2005; 7: pp. 52-58.
31. Giordano S.H.: Update on locally advanced breast cancer. Oncologist 2003; 8: pp. 521-530.
32. Pfleiderer S.O.R., Sachse S., Sauner D., et. al.: Changes in magnetic resonance mammography due to hormone replacement therapy. Breast Cancer Res 2004; 6: pp. R232-R238.
33. Rieber A., Nüssle K., Merkle E., et. al.: MR mammography: influence of menstrual cycle on the dynamic contrast enhancement of fibrocystic disease. Eur Radiol 1999; 9: pp. 1107-1112.
34. Schauer A., Korabiowska M., Kellner S., et. al.: Grading system for breast cancer. Anticancer Res 1998; 18: pp. 2139-2144.
35. American College of Radiology (ACR): Breast imaging reporting and data system (BI-RADS) atlas.2003.American College of RadiologyReston, VA
36. Fischer D.R., Baltzer P., Malich A., et. al.: Is the “blooming sign” a promising additional tool to determine malignancy in MR mammography?. Eur Radiol 2004; 14: pp. 394-401.
37. Penn A., Thompson S., Brem R., et. al.: Morphologic blooming in breast MRI as a characterization of margin for discriminating benign from malignant lesions. Acad Radiol 2006; 13: pp. 1344-1354.
38. Buadu L.D., Murakami J., Murayama S., et. al.: Breast lesions: correlation of contrast medium enhancement patterns on MR images with histopathologic findings and tumor angiogenesis. Radiology 1996; 200: pp. 639-649.
39. Renz D.M., Baltzer P.A.T., Böttcher J., et. al.: New signs of tumors in magnetic resonance imaging. Eur Radiol 2006; 16: pp. E80-E82.
40. Macéa J.R., Fregnani J.H.T.G.: Anatomy of the thoracic wall, axilla and breast. Int J Morphol 2006; 24: pp. 691-704.
41. Mahfouz A.E., Sherif H., Saad A., et. al.: Gadolinium-enhanced MR angiography of the breast: is breast cancer associated with ipsilateral higher vascularity?. Eur Radiol 2001; 11: pp. 965-969.
42. Droulias C.A., Sewell C.W., McSweeney M.B., et. al.: Inflammatory carcinoma of the breast: a correlation of clinical, radiologic and pathologic findings. Ann Surg 1976; 184: pp. 217-222.
43. Guinebretière J.M., Menet E., Tardivon A., et. al.: Normal and pathological breast, the histological basis. Eur J Radiol 2005; 54: pp. 6-14.
44. Dirix L.Y., Dam P.V., Prové A., et. al.: Inflammatory breast cancer: current understanding. Curr Opin Oncol 2006; 18: pp. 563-571.
45. Dvorak H.F., Dickersin G.R., Dvorak A.M., et. al.: Human breast carcinoma: fibrin deposits and desmoplasia. J Natl Cancer Inst 1981; 67: pp. 335-345.
46. Brown L.F., Guidi A.J., Schnitt S.J., et. al.: Vascular stroma formation in carcinoma in situ, invasive carcinoma, and metastatic carcinoma of the breast. Clin Cancer Res 1999; 5: pp. 1041-1056.
47. Van Goethem M., Tjalma W., Schelfout K., et. al.: Magnetic resonance imaging in breast cancer. Eur J Surg Oncol 2006; 32: pp. 901-910.
48. Crowe D.J., Helvie M.A., Wilson T.E.: Breast infection. Invest Radiol 1995; 30: pp. 582-587.