
Informatics methods and systems in support of clinical care are well established in the health care enterprise. The new paradigm of patient-centered radiology creates new requirements and challenges that can be enabled by informatics. In particular, computer support can help referring physicians tailor their imaging requests to those procedures that would be most helpful for their patients’clinical context. Informatics methods can assist radiologists in recognizing important findings in images as well as helping them decide the best course of action for patients given the radiologic imaging results and other clinical data. Finally, informatics methods can help engage patients in their care by providing information about their imaging procedures and results. All of these informatics technologies share in common the ability to bring together critical knowledge filtered according to the specific requirements of patients undergoing radiologic imaging, a key component of patient-centered radiology. The goals of this article are to review the opportunities for informatics in supporting patient-centered radiology, to demonstrate the potential utility of these methods, and to point radiologists to the ways that informatics will help them provide care that is tailored to each patient.
Patient-centered radiology is a topic of increasing importance in radiology, motivated by both physicians and patients. From the physician perspective, patient-centered radiology is being driven by the rapidly evolving medical and molecular knowledge that promises personalized medicine . Patients are also driving patient-centered radiology, with increasing expectations of accessing and reviewing their medical information and participating more actively in their care . Patient-centered radiology practice is crucial, affecting the visibility of radiologists in health care .
The patient-centered radiology paradigm brings important challenges to both physicians and patients. From the physician perspective, two important challenges are selecting the appropriate imaging procedure for specific patients and rendering the best imaging interpretation that is personalized to the particular patient (eg, by incorporating historical and clinical data). In selecting an imaging procedure for specific patients, radiologists have an increasing number of choices. There are many new diagnostic agents and imaging techniques, increasingly tailored on the basis of patient-specific information. Radiology is evolving from generic imaging protocols for broad categories of indications to specific, often complex, image acquisition protocols designed to answer specific clinical questions. Radiology procedures and the selection of imaging agents will be increasingly customized according to each patient’s underlying or suspected disease process, particularly in the era of molecular imaging.
Rendering the best patient-specific imaging interpretation is another requirement for radiologists in the patient-centered radiology paradigm. The pace of discovery in radiology is rapid, and radiologists are challenged by the information explosion and their ability to keep pace with the latest knowledge that could affect their imaging interpretations. Tools are needed to help radiologists access and use current knowledge, to guide them in customizing imaging to each patient, and to help them render the most accurate diagnoses.
From the patient perspective in patient-centered radiology, the expectation is that they will assume active roles in their care, particularly being informed about the results of imaging procedures and participating in medical decision making after receiving those results. Patients, like physicians, are overwhelmed by the amount of information related to imaging available online from diverse sources of questionable validity, and they are looking for help. Informing patients about the diagnostic imaging options available as well as the results of their studies is a crucial way radiologists can help patients to be engaged in their care as well as to ensure that critical results are communicated to them. This is a particularly important opportunity because the volume of information in physician practices and the lack of systems to manage the flow of information sometimes result in delayed communication of results from referring physician to patients . Radiologists can adopt informatics methods to manage the information glut and can help communicate results to patients. At the same time, radiologists will become more visible in the care process and make patients aware that radiologists serve an integral role in patient care.
A second aspect of the patient perspective in patient-centered radiology is enabling patients to participate in the medical decision-making process. Just as personalized medicine is changing how radiologists will approach interpreting images, shared decision making personalizes the patient management process. In many cases, the results of imaging are suggestive, but not conclusive, for disease. The choice of next steps (additional imaging, biopsy, or watchful waiting) often is affected by patient preferences. Shared medical decision making permits patients to weigh the trade-offs in their utility of the different outcomes, the likelihood of each outcome, and their risk tolerance.
Get Radiology Tree app to read full this article<
 Open full size image
Open full size image
Figure 1
Informatics aspects supporting patient-centered radiology. Informatics supports patient-centered radiology throughout the imaging work flow, in aspects of care that involve the radiologist (dashed boxes) and the patient (dotted boxes) , beginning with the imaging request (just-in-time appropriateness methods), followed by the radiologist’s interpreting the images (diagnostic decision support systems), and finally by ensuring that the patient is informed of the imaging results (results communication systems) and is involved in the subsequent management decisions (shared decision making).
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
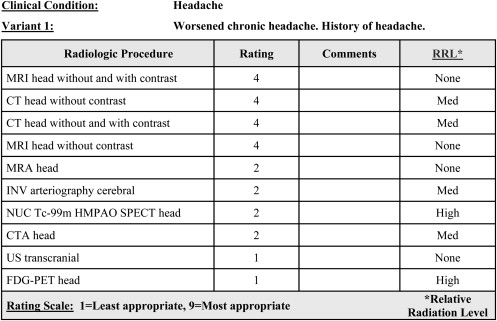
Guidance for procedure appropriateness
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Defining and Encoding Guidelines for Imaging
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Order Entry Decision Support
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
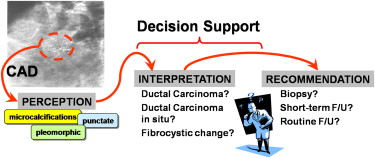
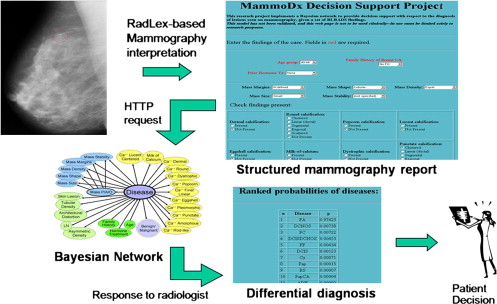
Diagnostic decision support for interpretation
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results communcation and shared decision making
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
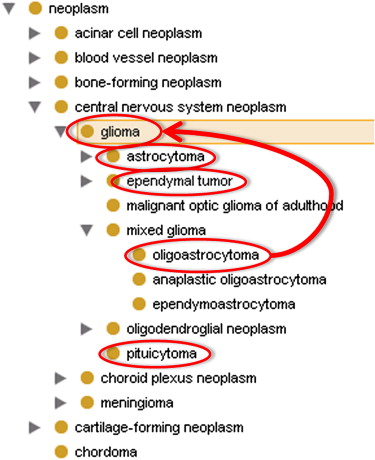
Structured Reporting and Controlled Terminology
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Electronic Notification and Reminder Systems
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Shared Decision Making
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Conclusion
Get Radiology Tree app to read full this article<
Acknowledgment
Get Radiology Tree app to read full this article<
References
1. Thrall J.H.: Personalized medicine. Radiology 2004; 231: pp. 613-616.
2. Ortega D., Garcia C.: Communication between radiologists and patients: an unsolved issue. J Am Coll Radiol 2006; 3: pp. 472-477.
3. Ruiz J.A., Glazer G.M.: The state of radiology in 2006: very high spatial resolution but no visibility. Radiology 2006; 241: pp. 11-16.
4. Kolata G. Sick and scared, and waiting, waiting, waiting. The New York Times. August 20, 2005:A1.
5. Sistrom C.L.: In support of the ACR Appropriateness Criteria. J Am Coll Radiol 2008; 5: pp. 630-635.
6. Cascade P.N.: The American College of Radiology. ACR Appropriateness Criteria project. Radiology 2000; 214: pp. 3-46.
7. Jordan J.E., Seidenwurm D.J., Davis P.C., et. al.: Expert Panel on Neurologic Imaging. Headache. ACR Appropriateness Criteria.2006.American College of RadiologyReston, VA
8. Khajouei R., Jaspers M.W.: CPOE system design aspects and their qualitative effect on usability. Stud Health Technol Inform 2008; 136: pp. 309-314.
9. Agency for Healthcare Research and Quality. National Guideline Clearinghouse. Available at: http://www.guideline.gov . Accessed October 24, 2008.
10. Kawahara N.E., Jordan F.M.: Influencing prescribing behavior by adapting computerized order-entry pathways. Am J Hosp Pharm 1989; 46: pp. 1798-1801.
11. Niazkhani Z, van der Sijs H, Pirnejad H, Redekop WK, Aarts J. Same system, different outcomes: comparing the transitions from two paper-based systems to the same computerized physician order entry system. Int J Med Inform. In press.
12. Rosenthal D.I., Weilburg J.B., Schultz T., et. al.: Radiology order entry with decision support: initial clinical experience. J Am Coll Radiol 2006; 3: pp. 799-806.
13. Khorasani R.: Computerized physician order entry and decision support: improving the quality of care. Radiographics 2001; 21: pp. 1015-1018.
14. Doi K.: Computer-aided diagnosis in medical imaging: historical review, current status and future potential. Comput Med Imaging Graph 2007; 31: pp. 198-211.
15. Siegle R.L., Baram E.M., Reuter S.R., Clarke E.A., Lancaster J.L., McMahan C.A.: Rates of disagreement in imaging interpretation in a group of community hospitals. Acad Radiol 1998; 5: pp. 148-154.
16. Barlow W.E., Chi C., Carney P.A., et. al.: Accuracy of screening mammography interpretation by characteristics of radiologists. J Natl Cancer Inst 2004; 96: pp. 1840-1850.
17. McDonald C.J.: Medical heuristics: the silent adjudicators of clinical practice. Ann Intern Med 1996; 124: pp. 56-62.
18. Burnside E., Rubin D., Shachter R.: A Bayesian network for mammography. Proc AMIA Symp 2000; pp. 106-110.
19. Burnside E.S., Rubin D.L., Fine J.P., Shachter R.D., Sisney G.A., Leung W.K.: Bayesian network to predict breast cancer risk of mammographic microcalcifications and reduce number of benign biopsy results: initial experience. Radiology 2006; 240: pp. 666-673.
20. Burnside E.S., Rubin D.L., Shachter R.D.: Using a Bayesian network to predict the probability and type of breast cancer represented by microcalcifications on mammography. Stud Health Technol Inform 2004; 107: pp. 13-17.
21. Burnside E.S., Rubin D.L., Shachter R.D., Sohlich R.E., Sickles E.A.: A probabilistic expert system that provides automated mammographic-histologic correlation: initial experience. AJR Am J Roentgenol 2004; 182: pp. 481-488.
22. Berlin L.: Communicating radiology results. Lancet 2006; 367: pp. 373-375.
23. Poon E.G., Haas J.S., Louise Puopolo A., et. al.: Communication factors in the follow-up of abnormal mammograms. J Gen Intern Med 2004; 19: pp. 316-323.
24. Renfrew D.L., Franken E.A., Berbaum K.S., Weigelt F.H., Abu-Yousef M.M.: Error in radiology: classification and lessons in 182 cases presented at a problem case conference. Radiology 1992; 183: pp. 145-150.
25. Braeuning M.P., Earp J.L., O’Brien S.M., et. al.: Informing patients of diagnostic mammography results: mammographer’s opinions. Acad Radiol 2000; 7: pp. 335-340.
26. American College of Radiology: ACR practice guideline for communication of diagnostic imaging findings. Practice Guidelines & Technical Standards.2005.American College of RadiologyReston, VA
27. Berlin L. Communication of radiologic findings: is the landscape changing? Imaging Econ. 2005. Available at: http://www.imagingeconomics.com/library/200509-06.asp . Accessed October 24, 2008.
28. Sasson J.P., Zand T., Lown B.A.: Communication in the diagnostic mammography suite: implications for practice and training. Acad Radiol 2008; 15: pp. 417-424.
29. Lafortune M., Breton G., Baudouin J.L.: The radiological report: what is useful for the referring physician?. Can Assoc Radiol J 1988; 39: pp. 140-143.
30. Khorasani R., Bates D.W., Teeger S., Rothschild J.M., Adams D.F., Seltzer S.E.: Is terminology used effectively to convey diagnostic certainty in radiology reports?. Acad Radiol 2003; 10: pp. 685-688.
31. Sistrom C.L., Langlotz C.P.: A framework for improving radiology reporting. J Am Coll Radiol 2005; 2: pp. 159-167.
32. Liu D., Zucherman M., Tulloss W.B.: Six characteristics of effective structured reporting and the inevitable integration with speech recognition. J Digit Imaging 2006; 19: pp. 98-104.
33. Sobel J.L., Pearson M.L., Gross K., et. al.: Information content and clarity of radiologists’ reports for chest radiography. Acad Radiol 1996; 3: pp. 709-717.
34. Stearns M.Q., Price C., Spackman K.A., Wang A.Y.: SNOMED clinical terms: overview of the development process and project status. Proc AMIA Symp 2001; pp. 662-666.
35. Langlotz C.P.: RadLex: a new method for indexing online educational materials. Radiographics 2006; 26: pp. 1595-1597.
36. Rubin D.L., Noy N.F., Musen M.A.: Protege: a tool for managing and using terminology in radiology applications. J Digit Imaging 2007; 20: pp. 34-46.
37. Halsted M.J., Froehle C.M.: Design, implementation, and assessment of a radiology workflow management system. AJR Am J Roentgenol 2008; 191: pp. 321-327.
38. Johnson A.J., Hawkins H., Applegate K.E.: Web-based results distribution: new channels of communication from radiologists to patients. J Am Coll Radiol 2005; 2: pp. 168-173.
39. Juluru K., Eng J.: Internet-based radiology order-entry, reporting, and workflow management system for coordinating urgent study requests during off-hours. AJR Am J Roentgenol 2005; 184: pp. 1017-1020.
40. Stoltz C. Microsoft Health vs. Google Health. The Washington Post. March 11, 2008. Available at: http://www.washingtonpost.com/wp-dyn/content/article/2008/03/10/AR2008031001532.html . Accessed October 24, 2008.
41. Mendelson D.S., Bak P.R., Menschik E., Siegel E.: Informatics in radiology: image exchange: IHE and the evolution of image sharing. Radiographics 2008; 28: pp. 1817-1833.
42. Chan E.C.: Promoting an ethical approach to unproven screening imaging tests. J Am Coll Radiol 2005; 2: pp. 311-320.