
Rationale and Objectives
Contrast-enhanced digital mammography and digital breast tomosynthesis are two imaging techniques that attempt to increase malignant breast lesion conspicuity. The combination of these into a single technique, contrast-enhanced digital breast tomosynthesis (CE-DBT), could potentially integrate the strengths of both. The objectives of this study were to assess the clinical feasibility of CE-DBT as an adjunct to digital mammography, and to correlate lesion enhancement characteristics and morphology obtained with CE-DBT to digital mammography, ultrasound, and magnetic resonance (MR).
Materials and Methods
CE-DBT (GE Senographe 2000D; Milwaukee, WI) was performed as a pilot study in an ongoing National Cancer Institute–funded grant (P01-CA85484) studying multimodality breast imaging. Thirteen patients with ACR BI-RADS category 4 or 5 breast lesions underwent imaging with digital mammography, ultrasound, MR, and CE-DBT. CE-DBT was performed at 49 kVp with a rhodium target and a 0.27-mm copper (Alfa Aesar, Ward Hill, MA) filter. Preinjection and postinjection DBT image sets were acquired in the medial lateral oblique projection with slight compression. Each image set consists of nine images acquired over a 50-degree arc and was obtained with a mean glandular x-ray dose comparable to two conventional mammographic views. Between the precontrast and postcontrast DBT image sets, a single bolus of iodinated contrast agent (1 ml/kg at 2 ml/s, Omnipaque-300; Amersham Health Inc., Princeton, NJ) was administered. Images were reconstructed using filtered-backprojection in 1-mm increments and transmitted to a clinical PACS workstation.
Results
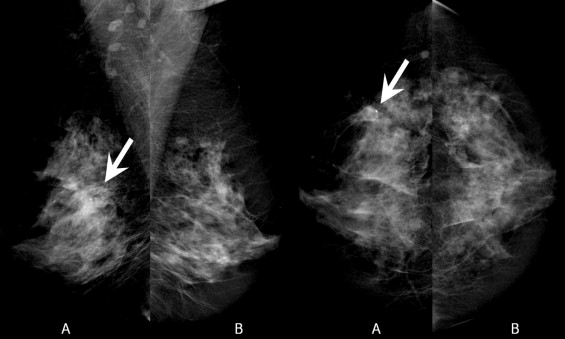
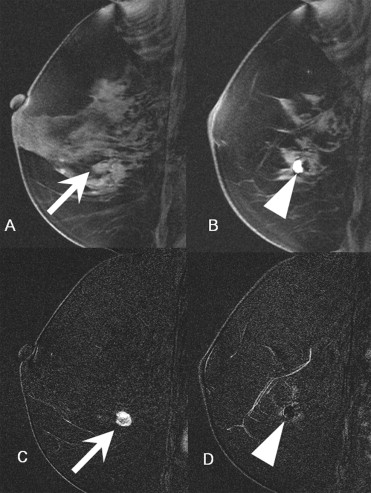
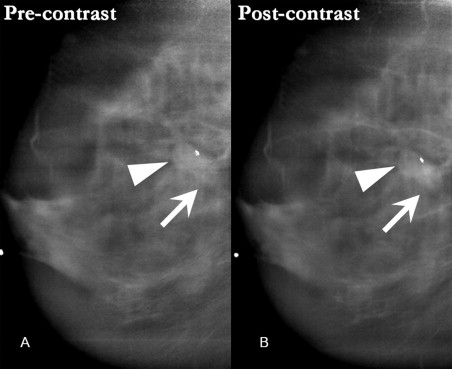
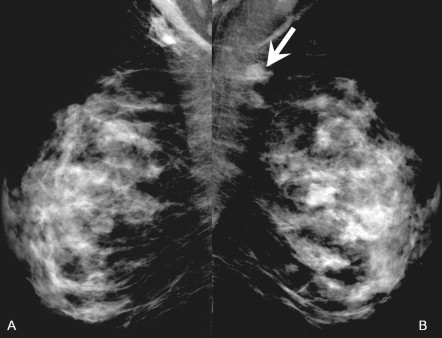
Initial experience suggests that CE-DBT provides morphologic and vascular characteristics of breast lesions qualitatively concordant with that of digital mammography and MR.
Conclusion
As an adjunct to digital mammography, CE-DBT may be a potential alternative tool for breast lesion morphologic and vascular characterization.
Vascular neoangiogenesis has been shown to be essential for breast cancer growth ( ). Malignant breast tumor angiogenesis factors stimulate formation of disorganized vessel networks with abnormally increased vessel permeability ( ). As a result, the enhancement pattern of breast cancers with vascular contrast agents often differs from that of benign and normal breast tissues. This aspect of breast cancer biology has been most extensively illustrated with gadolinium-enhanced breast magnetic resonance (MR), which when applied clinically provides vascular characterization of breast lesions ( ).
X-ray techniques combined with contrast agents are also able to demonstrate this feature of breast cancer biology, as has been illustrated with digital subtraction angiography of the breast ( ) and contrast-enhanced CT of the breast ( ). Jong et al. ( ), Lewin et al. ( ), and Diekmann et al. ( ) have demonstrated that enhancement of breast cancers can be detected with contrast-enhanced digital mammography and that this technique can increase mammographic lesion conspicuity.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Materials and methods
Patient Population
Get Radiology Tree app to read full this article<
Technique
Get Radiology Tree app to read full this article<
Imaging System
Get Radiology Tree app to read full this article<
Image Acquisition
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Image Processing and Reconstruction
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 1
Multimodality Imaging and Pathology Results
CE-DBT Case No. Column data Side Digital Mammography Ultrasound MR Pathology Precontrast DBT Postcontrast DBT 1 Left 9-mm group of calcifications; status post–core biopsy. 10 × 12 × 9 mm hypoechoic mass. 11-mm enhancing lesion; adjacent hematoma Infiltrating ductal carcinoma, 1.8 cm; biopsy site reaction Rounded density adjacent to biopsy clip Enhancing mass adjacent to postbiopsy seroma/hematoma 2 Left Focal asymmetry with 12-mm cluster of heterogeneous calcifications. Negative Negative Usual ductal hyperplasia without atypia Negative Negative 3 Right 3.2-cm focal asymmetry Multiple solid vascular masses 3.5-cm area of clumped enhancement Invasive ductal carcinoma Multiple masses Segmental, clumped enhancement 4 Right Postlumpectomy changes. Residual calcifications at margin. Postlumpectomy seroma 5-mm enhancing nodule at edge of seroma DCIS Seroma; otherwise negative Clumped enhancement at edge of seroma 5 Right 1.4-cm ill-defined asymmetry Irregular solid mass 1.3-cm enhancing mass Infiltrating ductal carcinoma Spiculated mass Enhancing spiculated mass 6 Left Two masses (1.6 cm and 3 cm), index lesion with biopsy clip Two irregular masses Two adjacent enhancing masses (combined size of 4.3 cm). Invasive ductal carcinoma Two adjacent masses Two enhancing masses 7 Right Postexcisional biopsy seroma Postexcisional biopsy seroma Clumped enhancement posterior to seroma 7.5 × 3.6 × 5.0-cm postbiopsy cavity; residual intraductal carcinoma Postexcisional biopsy seroma Enhancement posterior to seroma 8 Left Calcifications on film-screen only; digital mammogram negative 8-mm mass in medial breast Small mass with adjacent focus of enhancement in medial breast Invasive ductal carcinoma with DCIS No calcifications demonstrated Small foci of enhancement in central breast 9 Right Negative 2-cm mass in central breast; retroareolar fibroadenoma Enhancing 2-cm mass in central breast; retroareolar fibroadenoma Intraductal papilloma No suspicious finding No suspicious finding 10 Left 7-cm region of pleomorphic calcifications in lateral breast Large mass in lateral breast Large enhancing mass Extensive DCIS Large mass in upper outer quadrant Enhancing irregular mass in upper outer quadrant 11 Left 3.6-cm lobular mass in superior breast 3.6-cm lobular mass Enhancing 3.6-cm lobular mass Invasive lobular carcinoma Lobulated mass in upper breast Enhancing lobulated mass in upper breast 12 Right Postbiopsy changes; calcifications in superior and lateral breast Postbiopsy changes Postbiopsy changes DCIS at margins of postbiopsy cavity Postbiopsy changes Postbiopsy changes 13 Left Small mass in upper outer quadrant Mass in lateral breast 10 × 9 mm enhancing mass in lateral breast Invasive ductal carcinoma with DCIS Biopsy clip Small focus of faint enhancement adjacent to biopsy clip
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Rationale for Technical Parameters
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Future directions for technical optimization
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Clinical context
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Practical applications
Get Radiology Tree app to read full this article<
Acknowledgments
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Weidner N., Semple J.P., Welch W.R., et. al.: Tumor angiogenesis and metastasis: Correlation in invasive breast carcinoma. N Engl J Med 1991; 324: pp. 1-8.
2. Boetes C., Barentsz J.O., Mus R.D., et. al.: MR characterization of suspicious breast lesions with a gadolinium-enhanced TurboFLASH subtraction technique. Radiology 1994; 193: pp. 777-781.
3. Kaiser W.A., Zeitler E.: MR imaging of the breast: Fast imaging sequences with and without Gd-DTPA. Radiology 1989; 170: pp. 681-686.
4. Mussurakis S., Buckley D.L., Bowsley S., et. al.: Dynamic contrast-enhanced magnetic resonance imaging of the breast combined with pharmacokinetic analysis of gadolinium-DTPA uptake in the diagnosis of local recurrence of early stage breast carcinoma. Investig Radiol 1995; 30: pp. 650-662.
5. Sardanelli F., Rescinito G., Giordano G.D., et. al.: MR dynamic enhancement of breast lesions: High temporal resolution during the first-minute versus eight-minute study. J Comput Assist Tomogr 2000; 24: pp. 724-731.
6. Ackerman L.V., Watt A.C., Shetty P., et. al.: Breast lesions examined by digital angiography. Radiology 1985; 155: pp. 65-68.
7. Watt A.C., Ackerman L.V., Windham J.P., et. al.: Breast lesions: Differential diagnosis using digital subtraction angiography. Radiology 1986; 159: pp. 39-42.
8. Chang J., Nesbit D.E., Fisher D.R., et. al.: Computed tomographic mammography using a conventional body scanner. AJR Am J Roentgenol 1982; 138: pp. 553-558.
9. Sibala J.L., Chang J., Lin F., et. al.: Computed tomographic mammography. Arch Surg 1981; 116: pp. 114-117.
10. Lindfors K., Boone J., Nelson T., et. al.: 2005.Presented at the RSNA 91st Scientific Assembly and Annual MeetingChicago November 27–December 2
11. Yamamoto A., Fukushima H., Okamura R.: Dynamic helical CT mammography of breast cancer. Radiat Med 2006; 24: pp. 35-40.
12. Jong R.A., Yaffe M.J., Skarpathiotakis M., et. al.: Contrast-enhanced digital mammography: Initial clinical experience. Radiology 2003; 228: pp. 842-850.
13. Lewin J.M., Isaacs P.K., Vance V., et. al.: Dual-energy contrast-enhanced digital subtraction mammography: Feasibility. Radiology 2003; 229: pp. 261-268.
14. Diekmann F., Diekmann S., Jeunehomme F., et. al.: Digital mammography using iodine-based contrast media: Initial clinical experience with dynamic contrast medium enhancement. Invest Radiol 2005; 40: pp. 397-404.
15. Rafferty EA. Tomosynthesis: New weapon in breast cancer fight. Decis Imaging Econ 2004: 17. Available at http://www.imagingeconomics.com/library/200404-12.asp (accessed on April 17, 2006).
16. American College of Radiology (ACR): BI-RADS: Mammography.4ht ed.2003.American College of RadiologyReston, VA
17. Skarpathiotakis M., Yaffe M.J., Bloomquist A.K., et. al.: Development of contrast digital mammography. Med Physics 2002; 29: pp. 2419-2426.
18. Niklason L.T., Christian B.T., Niklason L.E., et. al.: Digital tomosynthesis in breast imaging. Radiology 1997; 205: pp. 399-406.
19. Carton A.-K., Li J., Albert M., Chen S., et. al.: Quantification for contrast-enhanced digital breast tomosynthesis.Flynn M.J.Hsieh J.Medical Imaging 2006: Physics of Medical Imaging.2006.(SPIE, Bellingham, WA)San Diego:pp. 111-121.
20. Boone J.M.: Normalized glandular dose (DgN) coefficients for arbitrary x-ray spectra in mammography: Computer-fit values of Monte Carlo derived data. Med Physics 2002; 29: pp. 869-875.
21. Boone J.M., Fewell T.R., Jennings R.J.: Molybdenum, rhodium, and tungsten anode spectral models using interpolating polynomials with application to mammography. Med Physics 1997; 24: pp. 1863-1874.
22. Maidment A.D.A., Albert M., Thunberg S., et. al.: Evaluation of a Photon-Counting Breast Tomosynthesis Imaging System.Flynn M.J.SPIE.2005.(SPIE, Bellingham, WA)San Diego, CA:pp. 572-582.
23. Rafferty E.A., Kopans D.B., Wu T., et. al.: 2004.Presented at the RSNA 90th Scientific Assembly and Annual MeetingChicago November 28–December 3
24. Stack J.P., Redmond O.M., Codd M.B., et. al.: Breast disease: Tissue characterization with Gd-DTPA enhancement profiles. Radiology 1990; 174: pp. 491-494.
25. Flickinger F.W., Allison J.D., Sherry R.M., et. al.: Differentiation of benign from malignant breast masses by time-intensity evaluation of contrast enhanced MRI. Magn Reson Imaging 1993; 11: pp. 617-620.
26. Buckley D.L., Mussurakis S., Horsman A.: Effect of temporal resolution on the diagnostic efficacy of contrast-enhanced MRI in the conservatively treated breast. J Comput Assist Tomogr 1998; 22: pp. 47-51.
27. Kuhl C.K., Mielcareck P., Klaschik S., et. al.: Dynamic breast MR imaging: Are signal intensity time course data useful for differential diagnosis of enhancing lesions?. Radiology 1999; 211: pp. 101-110.
28. Hylton N.: Vascularity assessment of breast lesions with gadolinium-enhanced MR imaging. Magn Reson Imaging Clin North Am 2001; 9: pp. 321-332.
29. Marx C., Facius M., Muller S., et. al.: Contrast enhanced digital mammography (CEDM): Phantom experiment and first clinical results.Antonuk L.E.Yaffe L.E.Medical Imaging 2002: Physics of Medical Imaging.2002.(SPIE, Bellingham, WA)San Diego:pp. 174-181.