
Rationale and Objectives
Intraductal papillary mucinous neoplasms (IPMNs) are precancerous lesions of the pancreas. Computed tomography (CT) has been recommended to screen the malignant potential of IPMNs. However, data evaluating the use of CT to differentiate categories of IPMN based on disease progression are limited. This study aimed to explore the correlation between CT characteristics and pathology in IPMN associated with invasive carcinoma.
Materials and Methods
A total of 31 patients with intraductal papillary mucinous carcinoma (IPMC) treated at one local regional hospital in Shanghai, China, were enrolled in this study. Patients were divided into two groups based on invasion component and characterized as follows: group A, an invasive component of less than 50% (IPMC-I); and group B, with invasion of 50% or greater and defined as pancreatic ductal adenocarcinoma associated with IPMN (PDAC-IPMN). First, we analyzed the imaging information of the 31 patients retrospectively. Then, we compared the imaging differences between the two groups.
Results
Fifteen patients with IPMC-1 and 16 patients with PDAC-IPMN were identified. There was no statistically significant difference in sex, age, lesion location, radiologic type, tumor size, mural nodule size, and lymphatic metastasis between the two groups. However, the arterial increased CT values were significantly different between the two groups ( P < .01), with values of 29.2 ± 12.4 HU for group A and 14.2 ± 8.8 HU for group B. The venous increased CT values were 44.6 ± 12.0 HU for group A and 28.4 ± 12.3 HU for group B, and these were significantly different between the two groups ( P < .01). In group A, 13 cases (86.7%) were classified as T1 or T2 stage, and in group B, eight cases (50.0%) were classified as T1 and T2 stage. There was a statistically significant difference in tumor classification between group A and group B patients ( P < .05).
Conclusions
IPMC-I and PDAC-IPMN have different characteristics in CT imaging, and we demonstrated that CT scans based on blood supply and lymphatic metastasis could be used to evaluate and potentially screen for variation in IPMC disease outcomes.
Introduction
Pancreatic intraductal papillary mucinous neoplasms (IPMNs) originate from the ductal epithelium with papillary proliferation and dilation of the main pancreatic duct or its major branches . IPMN is recognized as a premalignant lesion, which may progress from an adenoma to a carcinoma . Histologically, IPMNs are divided into four categories: IPMNs with (1) low-grade dysplasia, (2) moderate-grade dysplasia, (3) high-grade dysplasia, and (4) IPMNs associated with invasive carcinomas . Several studies have reported that approximately 4%–10% of individuals with IPMN develop pancreatic ductal adenocarcinoma (PDAC) . There is emerging evidence suggesting that biological behavior and long-term survival differ between patients diagnosed with IPMNs associated with invasive carcinomas and patients diagnosed with PDAC associated with IPMN .
According to the 2012 International Consensus Guidelines for the management of IPMNs and mucinous cystic neoplasm of the pancreas, computed tomography (CT) is recommended to screen the malignant potential of IPMNs and to distinguish IPMNs from other types of lesions . However, data that demonstrate that ability of CT to differentiate between IPMNs associated with invasive carcinomas and PDAC-associated IPMNs are limited. Compared with ultrasound, spiral CT and magnetic resonance imaging (MRI) can provide a clearer image. The diagnostic performance of multidetector CT and MRI for identifying the malignant potential of pancreatic IPMNs was similar . MRI has the advantages of no radiation and multiparameter imaging, but is expensive and takes a long time to scan. Spiral CT, with fewer relative contraindications and scanning speed and other characteristics, usually as the first line inspection, so we choose the spiral CT as a research tool for further research.
Get Radiology Tree app to read full this article<
Methods
Get Radiology Tree app to read full this article<
Pathologic Diagnosis
Get Radiology Tree app to read full this article<
TABLE 1
Patient Demographics and Intraductal Papillary Mucinous Neoplasm (IPMN) Pathologic Characteristics
Total ( n = 31) Age 63.0 ± 7.2 Sex (Male:Female) 2.4:1 Location, n (%) Head 18(58.1) Body 8(25.8) Tail 5(16.1) Radiologic type, n (%) Main duct type 28(90.3) Branch duct type 1(3.2) Mixed type 2(6.5) Degree of invasion, n (%) IPMC-I 15(48.4) IPMN associated with an invasive carcinoma 16(51.6) T stage, n (%) T1, T2 21(67.7) T3, T4 10(32.3) Lymphatic metastasis, n (%) 6(19.4)
IPMC-I, intraductal papillary mucinous carcinoma.
Get Radiology Tree app to read full this article<
CT Scanning
Get Radiology Tree app to read full this article<
Image Analysis
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Ethical Approval
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Results
CT Scanning
Get Radiology Tree app to read full this article<
TABLE 2
Patient Demographics and CT Characteristics Between IPMC-I and PDAC-PIMN Cases
IPMC-I ( n = 15) PDAC-IPMN ( n = 16)P Age 61.93 ± 7.89 63.94 ± 7.90 .486 Sex (Male:Female) 2.0:1 3.0:1 .454 CEA >5, n (%) 2(13.3) 3(18.8) .532 CA199 >37, n (%) 7(46.7) 10(62.5) .300 Location, n (%) .056 Head 12(80.0) 6(37.5) Body 2(13.3) 6(37.5) Tail 1(6.7) 4(25.0) Radiologic type, n (%) .616 Main duct type 14(93.3) 14(87.4) Branch duct type 1(6.7) 1(6.3) Mixed type 0 1(6.3) Tumor size, (mm) 46.7 ± 21.1 33.6 ± 13.9 .054 Wall size (mm) 12.6 ± 5.9 14.7 ± 7.3 .396 Main pancreatic duct diameter (mm) 10.2 ± 4.7 5.1 ± 3.6.003 Arterial increased CT value (HU) 29.2 ± 12.4 14.2 ± 8.8.001 Venous increased CT value (HU) 44.6 ± 12.0 28.4 ± 12.3.000 T stage, n (%).035 T1, T2 13(86.7) 8(50.0) T3, T4 2(13.3) 8(50.0) Lymphatic metastasis, n (%) 2(13.3) 4(25.0) .359
CA, carbohydrate antigen; CEA, carcino-embryonic antigen; CT, computed tomography; IPMC, intraductal papillary mucinous carcinoma; IPMN, intraductal papillary mucinous neoplasms; PDAC, pancreatic ductal adenocarcinoma.
Results of a Student t test are presented, and significant P values are in bold ( P < .05).
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
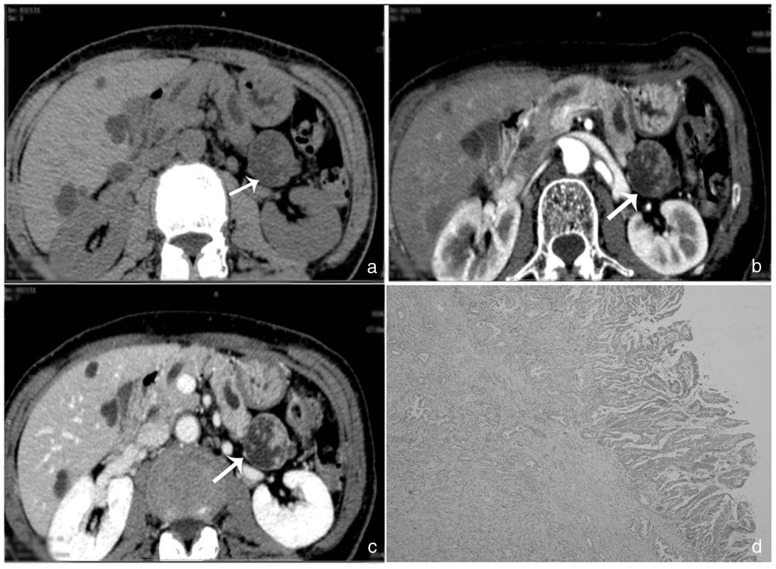
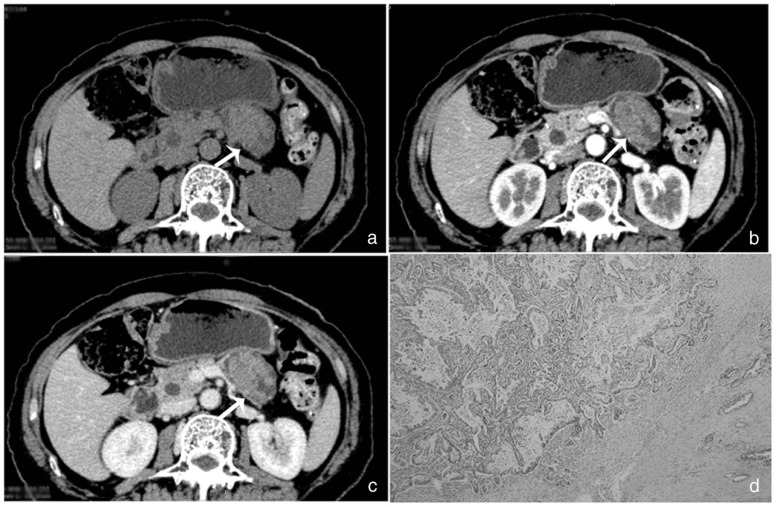
![Figure 3, (a) Computed tomography (CT) scans of the same individual in group A (intraductal papillary mucinous carcinoma [IPMC]-I); solid part of the lesions is papillary change, but duct dilation obviously. (b) CT scans of the same individual in group B (pancreatic ductal adenocarcinoma associated intraductal papillary mucinous neoplasms); lesions showed mild reinforcement, along the catheter infused to grow, but duct dilation not obviously.](https://storage.googleapis.com/dl.dentistrykey.com/clinical/IntraductalPapillaryMucinousNeoplasmsofthePancreas/2_1s20S1076633217300156.jpg)
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Conclusions
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Lim J.H., Lee G., Oh Y.L.: Radiologic spectrum of intraductal papillary mucinous tumor of the pancreas. Radiographics 2001; 21: pp. 323-337.
2. Kim S.H., Lee J.M., Lee E.S., et. al.: Intraductal papillary mucinous neoplasms of the pancreas: evaluation of malignant potential and surgical resectability by using MR imaging with MR cholangiography. Radiology 2015; 274: pp. 723-733.
3. Cooper C.L., O’Toole S.A., Kench J.G.: Classification, morphology and molecular pathology of premalignant lesions of the pancreas. Pathology 2013; 45: pp. 286-304.
4. Bosman F.T., Carneiro F., Hruban R.H., et. al.: WHO classification of tumours of the digestive system.2010.World Health OrganizationGeneva, Switzerland
5. Sahora K., Fernández-del Castillo C.: Intraductal papillary mucinous neoplasms. Curr Opin Gastroenterol 2015; 31: pp. 424-429.
6. Tamura K., Ohtsuka T., Date K., et. al.: Distinction of invasive carcinoma derived from intraductal papillary mucinous neoplasms from concomitant ductal adenocarcinoma of the pancreas using molecular biomarkers. Pancreas 2015; 00: pp. 1-10.
7. Kang M.J., Lee K.B., Jang J.Y., et. al.: Disease spectrum of intraductal papillary mucinous neoplasm with an associated invasive carcinoma invasive IPMN versus pancreatic ductal adenocarcinoma-associated IPMN. Pancreas 2013; 42: pp. 1267-1274.
8. Yamaguchi K., Ohuchida J., Ohtsuka T., et. al.: Intraductal papillary-mucinous tumor of the pancreas concomitant with ductal carcinoma of the pancreas. Pancreatology 2002; 2: pp. 484-490.
9. Yamaguchi K., Kanemitsu S., Hatori T., et. al.: Pancreatic ductal adenocarcinoma derived from IPMN and pancreatic ductal adenocarcinoma concomitant with IPMN. Pancreas 2011; 40: pp. 571-580.
10. Adsay V., Mino-Kenudson M., Furukawa T., et. al.: Pathologic evaluation and reporting of intraductal papillary mucinous neoplasms of the pancreas and other tumoral intraepithelial neoplasms of pancreatobiliary tract: recommendations of Verona Consensus Meeting. Ann Surg 2016; 263: pp. 162-177.
11. Tanaka M., Fernández-del Castillo C., Adsay V., et. al.: International consensus guidelines 2012 for the management of IPMN and MCN of the pancreas. Pancreatology 2012; 12: pp. 183-197.
12. Kang H.-J., Lee J.M., Joo I., et. al.: Assessment of malignant potential in intraductal papillary mucinous neoplasms of the pancreas: comparison between multi-detector CT and MR imaging with MR cholangiopancreatography. Radiology 2016; 000: pp. 1-12.
13. Bosman F.T., Carneiro F., Hruban R.H., et. al.: World Health Organization classification of tumors of the digestive system.4th ed.2010.IARCLyonpp. 304-313.
14. Tanaka M., Chari S., Adsay V., et. al.: International consensus guidelines for management of intraductal papillary mucinous neoplasms and mucinous cystic neoplasms of the pancreas. Pancreatology 2006; 6: pp. 17-32.
15. Edge S.B., Byrd D.R., Compton C.C., et. al.: AJCC cancer staging manual.7th ed.2010.Springer-VerlagNew York, NY
16. Tanaka M.: International consensus guidelines for management of intraductal papillary mucinous neoplasms and mucinous cystic neoplasms of the pancreas. Pancreatology 2006; 6: pp. 17-32.
17. Adsay N.V., Fukushima N., Furukawa T., et. al.: Intraductal neoplasm of the pancreas.Bosman F.T.Carneiro F.Hruban R.H. et. al.WHO classification of tumors of digestive system.2010.WHO PressLyon:pp. 304-313.
18. Japan Pancreas Society : Classification of pancreatic carcinoma.2nd English ed.2003.KaneharaTokyo
19. Hruban R.H., Takaori K., Klimstra D.S., et. al.: An illustrated consensus on the classification of pancreatic intraepithelial neoplasia and intraductal papillary mucinous neoplasms. Am J Surg Pathol 2004; 28: pp. 977-987.
20. Hruban R.H., Pitman M.B., Klimstra D.S.: Tumors of the pancreas.Silverberg S.G.AFIP Atlas of tumor pathology series 4.2007.ARP PressWashington, DC:pp. 75-110.
21. Hruban R.H.: An illustrated consensus on the classification of pancreatic intraepithelial neoplasia and intraductal papillary mucinous neoplasms. Am J Surg Pathol 2004; 28: pp. 977-987.
22. Dong Y.-W., Wang X.-P., Wu K.: Suppression of pancreatic carcinoma growth by activating peroxisome proliferator-activated receptor γ involves angiogenesis inhibition. World J Gastroenterol 2009; 15: pp. 441-448.
23. Linder S., Blasjo M., von Rosen A., et. al.: Pattern of distribution and prognostic value of angiogenesis in pancreatic duct carcinoma: a semiquantitative immunohistochemical study of 45 patients. Pancreas 2001; 22: pp. 240-247.
24. Fernández-del Castillo C.: Intraductal papillary mucinous neoplasms of the pancreas: a plea for prospective differentiation between main-duct and sidebranch tumors. Ann Surg Oncol 2005; 12: pp. 98-99.