
Rationale and Objectives
To prospectively test the hypothesis that transcatheter intraarterial perfusion magnetic resonance imaging (TRIP-MRI) measured semiquantitative perfusion reductions during transcatheter arterial chemoembolization of hepatocellular carcinoma (HCC) are associated with tumor response.
Materials and Methods
Twenty-eight patients (mean age 63 years; range 47–87 years) with 29 tumors underwent chemoembolization in a combined magnetic resonance interventional radiology suite. Intraprocedural tumor perfusion reductions during chemoembolization were monitored using TRIP-MRI. Pre- and postchemoembolization semiquantitative area under the time-signal enhancement curve (AUC) tumor perfusion was measured. Mean tumor perfusion pre- and postchemoembolization were compared using a paired t -test. Imaging follow-up was performed 1–3 months after chemoembolization. We studied the relationship between short-term tumor imaging response and intraprocedural perfusion reductions using univariate and multivariate analysis.
Results
Intraprocedural AUC perfusion value decreased significantly after chemoembolization (342.1 vs. 158.6 arbitrary unit, P < .001). Twenty-six patients with 27 HCCs ( n = 27) had follow-up imaging at mean 39 days postchemoembolization. Favorable response was present in 67% of these treated tumors according to necrosis criteria. Fifteen of 16 (94%) tumors with 25%–75% perfusion reductions showed necrosis treatment response compared to only 3 of 11 (27%) tumors with perfusion reductions outside the above range ( P = .001). Multivariate logistic regression indicated that intraprocedural tumor perfusion reduction and Child-Pugh class were independent factors associated significantly with tumor response ( P = .012 and .047, respectively).
Conclusion
TRIP-MRI can successfully measure semiquantitative changes in HCC perfusion during chemoembolization. Intraprocedural tumor perfusion reductions are associated with future tumor response.
Early identification of tumor response to transcatheter arterial chemoembolization may facilitate efficient assessment of treatment efficacy, timing of repeat therapy, and patient prognosis. Radiological hepatocellular carcinoma (HCC) response assessment by conventional computed tomography (CT) or magnetic resonance imaging (MRI) typically occurs 1–3 months after chemoembolization. Although several studies have identified early vascular and cellular changes using dynamic-contrast enhanced (DCE) and diffusion-weighted (DW) MRI as potential markers for early tumor response assessment , few studies have explored intraprocedural functional imaging biomarkers that may objectively predict future tumor response at the time of chemoembolization procedures.
Intraprocedural MRI allows objective assessment of tumor functions during transcatheter liver-directed embolotherapies . We previously demonstrated that transcatheter intraarterial perfusion (TRIP)-MRI, which uses direct catheter-based intraarterial injections of gadolinium (Gd) contrast, may be clinically employed for intraprocedural monitoring and quantification of tumor perfusion changes during chemoembolization when performed in a combined MRI/digital subtraction angiography (DSA) unit (termed MR-IR suite) . TRIP-MRI serially monitors tumor contrast uptake during chemoembolization, providing reliable objective measurement of tumor perfusion before and after therapy .
Get Radiology Tree app to read full this article<
Materials and methods
Get Radiology Tree app to read full this article<
Clinical Setting and Patients Characteristics
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 1
Patient Demographic and Tumor Characteristics
Characteristic Patient Number ( n = 28) Gender Male 21 Female 7 Age (y) Mean ± standard deviation 62.7 ± 10.4 HCC etiology Alcoholic 5 Hepatitis B virus 1 Hepatitis C virus 13 Other 9 AFP >200 ng/mL 8 ≤200 ng/mL 20 Child-Pugh class A 16 B 12 ECOG performance status 0 9 1 19 AJCC stage 1 17 2 5 3 6 Okuda stage 1 9 2 18 3 1 CLIP stage 0 7 1 11 2 7 3 1 4 2 Tumor morphology Unifocal 18 Multifocal 10 Distribution Unilobar 22 Bilobar 6 Size of targeted lesion (cm) Mean ± standard deviation 4.0 ± 2.7 Diagnosis method Biopsy 11 Imaging 17
AFP, alpha fetoprotein; AJCC, American Joint Committee on Cancer; CLIP, Cancer of the Liver Italian Program; ECOG, Eastern Cooperative Oncology Group.
Get Radiology Tree app to read full this article<
MR-IR Suite
Get Radiology Tree app to read full this article<
Chemoembolization Procedures
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Intraprocedural MRI
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
MRI Perfusion Data Analysis
Get Radiology Tree app to read full this article<
Tumor Response Evaluation
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Results
Intraprocedural TRIP-MRI
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Tumor Imaging Response
Get Radiology Tree app to read full this article<
Table 2
Tumor Imaging Response
Response CR PR SD PD WHO 0 0 25 2 Necrosis 7 11 7 2
CR, complete response; PD, progressive disease; PR, partial response; SD, stable disease; WHO, World Health Organization.
Get Radiology Tree app to read full this article<
Association between Intraprocedural Tumor Perfusion Reduction and Tumor Response
Get Radiology Tree app to read full this article<
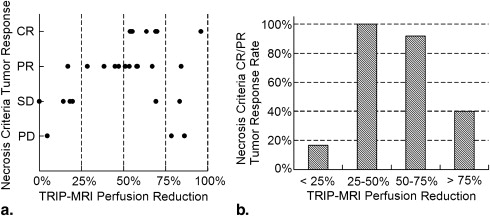
Table 3
Relationship Between Tumor Necrosis Imaging Response and MR Perfusion Reduction
Perfusion Reduction Necrosis Response CR PR SD PD Combined CR/PR Combined SD/PD <25% ( n = 6) 0 1 4 1 1 5 25%–50% ( n = 4) 0 4 0 0 4 0 50%–75% ( n = 12) 6 5 1 0 11 1 >75% ( n = 5) 1 1 1 2 2 3
CR, complete response; PD, progressive disease; PR, partial response; SD, stable disease.
Table 4
Analyses of Factors Associated with Tumor Response
Variable Necrosis Response_P_ -Value CR/PR ( n = 18, 67%) SD/PD ( n = 9, 23%) Univariate Analysis ∗ Multivariate Analysis † Perfusion reduction 0.001 0.012 25%–75% 15 (94%) 1 (6%) <25 or >75% 3 (27%) 8 (73%) Child-Pugh Class 0.004 0.047 A 13 (93%) 1 (7%) B 5 (38%) 8 (62%) Age (y) 1.000 ≤65 10 (67%) 5 (33%) >65 8 (67%) 4 (33%) Gender 0.653 Male 14 (70%) 6 (30%) Female 4 (57%) 3 (43%) Tumor size (cm) 0.683 ≤3.0 9 (75%) 3 (25%) >3.0 9 (60%) 6 (40%) Tumor number 0.692 1 10 (62.5%) 6 (37.5%) >1 8 (73%) 3 (27%) ECOG performance status 0.667 0 7 (78%) 2 (22%) > 0 11 (61%) 7 (39%) AJCC stage 0.683 1 9 (60%) 6 (40%) >1 9 (75%) 3 (25%) Serum AFP (ng/mL) 1.000 ≤200 13 (68%) 6 (32%) >200 5 (62.5%) 3 (37.5%) Serum bilirubin (mg/dL) 0.193 ≤1.3 8 (89%) 1 (11%) >1.3 10 (56%) 8 (44%)
AFP, alpha fetoprotein; AJCC, American Joint Committee on Cancer; CR, complete response; ECOG, Eastern Cooperative Oncology Group; PD, progressive disease; PR, partial response; SD, stable disease.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Kamel I.R., Bluemke D.A., Eng J., et. al.: The role of functional MR imaging in the assessment of tumor response after chemoembolization in patients with hepatocellular carcinoma. J Vasc Interv Radiol 2006; 17: pp. 505-512.
2. Chen C.Y., Li C.W., Kuo Y.T., et. al.: Early response of hepatocellular carcinoma to transcatheter arterial chemoembolization: choline levels and MR diffusion constants—initial experience. Radiology 2006; 239: pp. 448-456.
3. Kamel I.R., Liapi E., Reyes D.K., et. al.: Unresectable hepatocellular carcinoma: serial early vascular and cellular changes after transarterial chemoembolization as detected with MR imaging. Radiology 2009; 250: pp. 466-473.
4. Chung J.C., Naik N.K., Lewandowski R.J., et. al.: Diffusion-weighted magnetic resonance imaging to predict response of hepatocellular carcinoma to chemoembolization. World J Gastroenterol 2010; 16: pp. 3161-3167.
5. Wang D., Bangash A.K., Rhee T.K., et. al.: Liver tumors: monitoring embolization in rabbits with VX2 tumors–transcatheter intraarterial first-pass perfusion MR imaging. Radiology 2007; 245: pp. 130-139.
6. Lewandowski R.J., Wang D., Gehl J., et. al.: A comparison of chemoembolization endpoints using angiographic versus transcatheter intraarterial perfusion/MR imaging monitoring. J Vasc Interv Radiol 2007; 18: pp. 1249-1257.
7. Larson A.C., Wang D., Atassi B., et. al.: Transcatheter intraarterial perfusion (TRIP) – MRI monitoring of chemoembolization for hepatocellular carcinoma: feasibility of initial clinical translation. Radiology 2008; 246: pp. 964-971.
8. Gaba R.C., Wang D., Lewandowski R.J., et. al.: Four-dimensional transcatheter intraarterial perfusion MR imaging for monitoring chemoembolization of hepatocellular carcinoma: preliminary results. J Vasc Interv Radiol 2008; 19: pp. 1589-1595.
9. Wang D., Jin B., Lewandowski R.J., et. al.: Quantitative 4D Transcatheter intraarterial perfusion MRI for monitoring chemoembolization of hepatocellular carcinoma. J Magn Reson Imaging 2010; 31: pp. 1106-1116.
10. Bruix J., Sherman M., Llovet J.M., et. al.: Clinical management of hepatocellular carcinoma. Conclusions of the Barcelona – 2000 EASL conference. European Association for the Study of the Liver. J Hepatol 2001; 35: pp. 421-430.
11. Riaz A., Miller F.H., Kulik L.M., et. al.: Imaging response in the primary index lesion and clinical outcomes following transarterial locoregional therapy for hepatocellular carcinoma. JAMA 2010; 303: pp. 1062-1069.
12. Lewandowski R.J., Mulcahy M.F., Kulik L.M., et. al.: Chemoembolization for hepatocellular carcinoma: comprehensive imaging and survival analysis in a 172-patient cohort. Radiology 2010; 255: pp. 955-965.
13. World Health Organization: WHO handbook for reporting results of cancer treatment. Offset publication 48.1979.World Health OrganizationGeneva, Switzerland
14. Salem R., Lewandowski R.J., Kulik L., et. al.: Radioembolization results in longer time-to-progression and reduced toxicity compared with chemoembolization in patients with HCC. Gastroenterology 2011; 140: pp. 497-507.
15. Riaz A., Memon K., Miller F.H., et. al.: Role of EASL, RECIST and WHO response guidelines alone or in combination for hepatocellular carcinoma: radiologic-pathologic correlation. J Hepatol 2011; 54: pp. 695-704.
16. Riaz A., Ryu R.K., Kulik L.M., et. al.: Alpha-fetoprotein response after locoregional therapy for hepatocellular carcinoma: oncologic marker of radiologic response, progression, and survival. J Clin Oncol 2009; 27: pp. 5734-5742.
17. Dunfee B.L., Riaz A., Lewandowski R.J., et. al.: Yttrium-90 radioembolization for liver malignancies: prognostic factors associated with survival. J Vasc Interv Radiol 2010; 21: pp. 90-95.
18. Llovet J.M., Real M.I., Montana X., et. al.: Arterial embolisation or chemoembolisation versus symptomatic treatment in patients with unresectable hepatocellular carcinoma: a randomised controlled trial. Lancet 2002; 359: pp. 1734-1739.
19. Lo C.M., Ngan H., Tso W.K., et. al.: Randomized controlled trial of transarterial lipiodol chemoembolization for unresectable hepatocellular carcinoma. Hepatology 2002; 35: pp. 1164-1171.
20. Bruix J., Sherman M.: Practice Guidelines Committee, American Association for the Study of Liver Diseases. Management of hepatocellular carcinoma. Hepatology 2005; 42: pp. 1208-1236.
21. Ramsey D.E., Kernagis L.Y., Soulen M.C., et. al.: Chemoembolization of hepatocellular carcinoma. J Vasc Interv Radiol 2002; 13: pp. S211-S221.
22. Breedis C., Young G.: The blood supply of neoplasm of the liver. Am J Pathol 1954; 30: pp. 969-985.
23. Guo W.J., Li J., Chen Z., et. al.: Transient increased expression of VEGF and MMP-1 in a rat liver tumor model after hepatic arterial occlusion. Hepatogastroenterology 2004; 51: pp. 381-386.
24. Rhee T.K., Young J.Y., Larson A.C., et. al.: Effect of transcatheter arterial embolization on levels of hypoxia inducible factor-1 alpha in rabbit VX2 liver tumors. J Vasc Interv Radiol 2007; 18: pp. 639-645.
25. Brown D.B., Geschwind J.F., Soulen M.C., etal : Society of Interventional Radiology position statement on chemoembolization of hepatic malignancies. J Vasc Interv Radiol 2006; 17: pp. 217-223.
26. Bruix J., Sala M., Llovet J.M.: Chemoembolization for hepatocellular carcinoma. Gastroenterology 2004; 127: pp. S179-S188.
27. Soo C.S., Chuang V.P., Wallace S., et. al.: Treatment of hepatic neoplasm through extrahepatic collaterals. Radiology 1983; 147: pp. 45-49.
28. Charnsangavej C., Chuang V.P., Wallace S., et. al.: Angiographic classification of hepatic arterial collaterals. Radiology 1982; 144: pp. 485-494.
29. Lammer J., Malagari K., Vogl T., et. al.: Prospective Randomized Study of Doxorubicin-Eluting-Bead Embolization in the Treatment of Hepatocellular Carcinoma: Results of the PRECISION V Study. Cardiovasc Intervent Radiol 2010; 33: pp. 41-52.
30. Riaz A., Lewandowski R.J., Kulik L.: Radiologic-pathologic correlation of hepatocellular carcinoma treated with chemoembolization. Cardiovasc Intervent Radiol 2010; 33: pp. 1143-1152.
31. Jackson A., Haroon H., Zhu X.P., et. al.: Breath-hold perfusion and permeability mapping of hepatic malignancies using magnetic resonance imaging and a first-pass leakage profile model. NMR Biomed 2002; 15: pp. 164-173.
32. Wang D., Virmani S., Tang R., et. al.: Four-dimensional transcatheter intraarterial perfusion (TRIP)-MRI for monitoring liver tumor embolization in VX2 rabbits. Magn Reson Med 2008; 60: pp. 970-975.
33. Michels N.A.: Collateral arterial pathwas to the liver after ligation of the hepatic artery and removal of the celiac axis. Cancer 1953; 6: pp. 708-724.
34. Lewandowski R.J., Tepper J., Wang D., et. al.: MR imaging perfusion mismatch: a technique to verify successful targeting of liver tumors during transcatheter arterial chemoembolization. J Vasc Interv Radiol 2008; 19: pp. 698-705.
35. Llovet J.M.: Updated treatment approach to hepatocellular carcinoma. J Gastroenterol 2005; 40: pp. 225-235.