
Rationale and Objectives
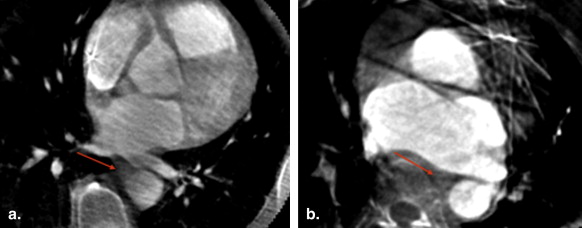
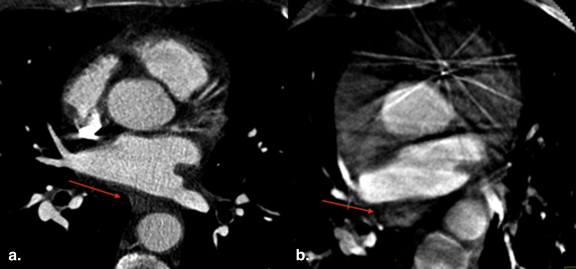
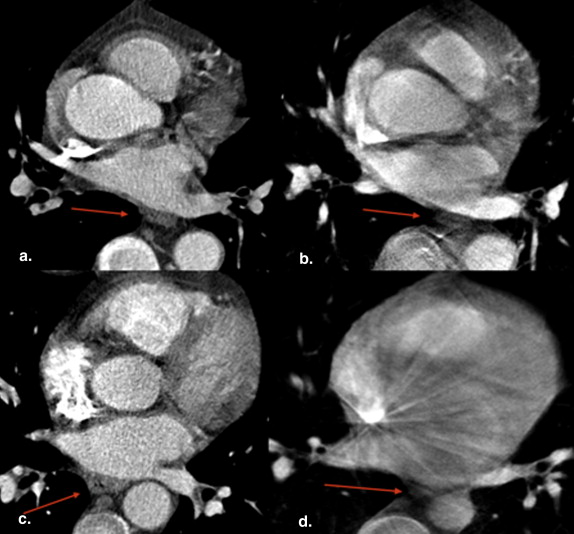
During radiofrequency catheter ablation for atrial fibrillation, the esophagus is at risk for thermal injury. In this study, C-arm computed tomography (CT) was compared to clinical CT, without the administration of oral contrast, to visualize the esophagus and its relationship to the left atrium and the ostia of the pulmonary veins (PVs) during the radiofrequency ablation procedure.
Materials and Methods
Sixteen subjects underwent both cardiac clinical CT and C-arm CT. Computed tomographic scans were performed on a multidetector scanner using a standard electrocardiographically gated protocol. C-arm computed tomographic scans were obtained using either a multisweep protocol with retrospective electrocardiographic gating or a non-gated single-sweep protocol. C-arm and clinical computed tomographic scans were analyzed in a random order and then compared for the following criteria: (1) visualization of the esophagus (yes or no), (2) relationship of esophageal position to the four PVs, and (3) direct contact or absence of a fat pad between the esophagus and the PV antrum.
Results
The esophagus was identified in all C-arm and clinical computed tomographic scans. In four cases, orthogonal planes were needed on C-arm CT (inferior PV level). In six patients, the esophageal location on C-arm CT was different from that on CT. Direct contact was reported in 19 of 64 of the segments (30%) examined on CT and in 26 of 64 (41%) on C-arm CT. In five of 64 segments (8%), C-arm CT overestimated a direct contact of the esophagus to the left atrium.
Conclusions
C-arm computed tomographic image quality without the administration of oral contrast agents was shown to be sufficient for visualization of the esophagus location during a radiofrequency catheter ablation procedure for atrial fibrillation.
Radiofrequency catheter ablation (RFCA) of atrial fibrillation has emerged as an important therapeutic option for patients refractory to antiarrhythmic medications. Although there are many approaches to the ablation of atrial fibrillation, isolation of the pulmonary veins (PVs) remains crucial for success of this procedure . Because the PVs are posterior structures, successful isolation requires ablation in the posterior left atrium (LA). In addition, RFCA may often be extended to other areas of the LA, in particular the posterior wall, the mitral isthmus, the atrial roof , and the interatrial septum .
Because of its proximity to the posterior wall of the LA, the esophagus may be at risk for thermal injury during RFCA . Atrioesophageal fistula has been reported in the literature as a rare event but one with a significantly high mortality rate.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Materials and methods
Patients
Get Radiology Tree app to read full this article<
Imaging Protocols
Cardiac CT
Get Radiology Tree app to read full this article<
Cardiac C-arm CT
Electrocardiographically gated protocol (13 subjects)
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Non-gated protocol (three subjects)
Get Radiology Tree app to read full this article<
Image Analysis
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Esophageal Visualization (Yes or No)
Get Radiology Tree app to read full this article<

Get Radiology Tree app to read full this article<
Localization and Proximity to a PV Antrum
Get Radiology Tree app to read full this article<

Get Radiology Tree app to read full this article<
Esophageal Movement
Get Radiology Tree app to read full this article<
Absence of Fat Pad (Direct Contact Between Esophagus and LA/PV Ostia)
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Visualization of the Esophagus
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Relationship of Esophagus and the LA
Get Radiology Tree app to read full this article<
Table 1
Esophageal Locations
Subject RSPV LSPV RIPV LIPV C-arm CT CT C-arm CT CT C-arm CT CT C-arm CT CT 1 3 ∗ 5 ∗ 3 3 4 4 6 6 2 5 ∗ 3 ∗ 5 5 4 4 6 ∗ 4 ∗ 3 5 5 5 5 4 4 4 4 4 5 5 5 5 6 6 6 6 5 5 5 5 5 4 ∗ 6 ∗ 4 ∗ 6 ∗ 6 5 5 5 5 6 6 6 6 7 1 ∗ 5 ∗ 1 ∗ 5 ∗ 2 ∗ 4 ∗ 2 ∗ 4 ∗ 8 3 3 3 3 4 4 4 4 9 5 5 5 5 6 6 6 6 10 5 5 5 5 6 6 6 6 11 3 3 3 3 4 4 4 4 12 5 5 5 5 6 6 6 6 13 5 5 5 5 6 6 6 6 14 5 5 5 5 6 6 6 6 15 5 5 5 5 2 ∗ 4 ∗ 6 ∗ 4 ∗ 16 5 ∗ 3 ∗ 5 ∗ 3 ∗ 6 ∗ 4 ∗ 6 6
CT, computed tomography; LIPV, left inferior pulmonary vein; LSPV, left superior pulmonary vein; RIPV, right inferior pulmonary vein; RSPV, right superior pulmonary vein.
The numbers in the boxes correspond to the anatomic areas where the esophagus was located on the axial plane at the level of each of the four main pulmonary veins.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Esophageal Movement
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Absence of Fat Pad (Direct Contact Between Esophagus and LA/PV Ostia)
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Conclusions
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Haissaguerre M., Jais P., Shah D.C., et. al.: Spontaneous initiation of atrial fibrillation by ectopic beats originating in the pulmonary veins. N Engl J Med 1998; 339: pp. 659-666.
2. Tsao H.M., Wu M.H., Higa S., et. al.: Anatomic relationship of the esophagus and left atrium: implication for catheter ablation of atrial fibrillation. Chest 2005; 128: pp. 2581-2587.
3. Jais P., Haissaguerre M., Shah D.C., et. al.: Regional disparities of endocardial atrial activation in paroxysmal atrial fibrillation. Pacing Clin Electrophysiol 1996; 19: pp. 1998-2003.
4. Wongcharoen W., Tsao H.M., Wu M.H., et. al.: Morphologic characteristics of the left atrial appendage, roof, and septum: implications for the ablation of atrial fibrillation. J Cardiovasc Electrophysiol 2006; 17: pp. 951-956.
5. Chiam P.T., Ruiz C.E.: Percutaneous transcatheter left atrial appendage exclusion in atrial fibrillation. J Invasive Cardiol 2008; 20: pp. E109-E113.
6. Pappone C., Oral H., Santinelli V., et. al.: Atrio-esophageal fistula as a complication of percutaneous transcatheter ablation of atrial fibrillation. Circulation 2004; 109: pp. 2724-2726.
7. Scanavacca M.I., D’Avila A., Parga J., et. al.: Left atrial-esophageal fistula following radiofrequency catheter ablation of atrial fibrillation. J Cardiovasc Electrophysiol 2004; 15: pp. 960-962.
8. Kottkamp H., Hindricks G., Autschbach R., et. al.: Specific linear left atrial lesions in atrial fibrillation: intraoperative radiofrequency ablation using minimally invasive surgical techniques. J Am Coll Cardiol 2002; 40: pp. 475-480.
9. Sonmez B., Demirsoy E., Yagan N., et. al.: A fatal complication due to radiofrequency ablation for atrial fibrillation: atrio-esophageal fistula. Ann Thorac Surg 2003; 76: pp. 281-283.
10. Cronin P., Sneider M.B., Kazerooni E.A., et. al.: MDCT of the left atrium and pulmonary veins in planning radiofrequency ablation for atrial fibrillation: a how-to guide. AJR Am J Roentgenol 2004; 183: pp. 767-778.
11. Cury R.C., Abbara S., Schmidt S., et. al.: Relationship of the esophagus and aorta to the left atrium and pulmonary veins: implications for catheter ablation of atrial fibrillation. Heart Rhythm 2005; 2: pp. 1317-1323.
12. Cummings J.E., Schweikert R.A., Saliba W.I., et. al.: Assessment of temperature, proximity, and course of the esophagus during radiofrequency ablation within the left atrium. Circulation 2005; 112: pp. 459-464.
13. Good E., Oral H., Lemola K., et. al.: Movement of the esophagus during left atrial catheter ablation for atrial fibrillation. J Am Coll Cardiol 2005; 46: pp. 2107-2110.
14. Pollak S.J., Monir G., Chernoby M.S., et. al.: Novel imaging techniques of the esophagus enhancing safety of left atrial ablation. J Cardiovasc Electrophysiol 2005; 16: pp. 244-248.
15. Al-Ahmad A., Wigstrom L., Sandner-Porkristl D., et. al.: Time-resolved three-dimensional imaging of the left atrium and pulmonary veins in the interventional suite—a comparison between multisweep gated rotational three-dimensional reconstructed fluoroscopy and multislice computed tomography. Heart Rhythm 2008; 5: pp. 513-519.
16. Mehdizadeh A, Fahrig R, Wang PJ, et al. Comparison of pulmonary veins and left atrial dimensions in humans using gated rotational cardiac fluoroscopy vs. cardiac CT. Presented at: American College of Cardiology 57th Annual Scientific Session; Chicago, IL; 2008.
17. Bongartz G., Golding S.J., Jurik G.A., et. al.: European guidelines on quality criteria for computed tomography.1999.European CommissionLuxembourg
18. Son HK, Lee SH, Nam S, et al. Radiation dose during CT scan with PET/CT clinical protocols. IEEE Nucl Sci Symp Conf Rec 2006; 4:2210-2214.
19. Wielandts J.Y., Smans K., Ector J., et. al.: Effective dose analysis of three-dimensional rotational angiography during catheter ablation procedures. Phys Med Biol 2010; 55: pp. 563-579.
20. Lauritsch G., Boese J., Wigstrom L., et. al.: Towards cardiac C-arm computed tomography. IEEE Trans Med Imaging 2006; 25: pp. 922-934.
21. Cummings J.E., Schweikert R.A., Saliba W.I., et. al.: Brief communication: atrial-esophageal fistulas after radiofrequency ablation. Ann Intern Med 2006; 144: pp. 572-574.
22. Lemola K., Sneider M., Desjardins B., et. al.: Computed tomographic analysis of the anatomy of the left atrium and the esophagus: implications for left atrial catheter ablation. Circulation 2004; 110: pp. 3655-3660.
23. Kenigsberg D.N., Lee B.P., Grizzard J.D., et. al.: Accuracy of intracardiac echocardiography for assessing the esophageal course along the posterior left atrium: a comparison to magnetic resonance imaging. J Cardiovasc Electrophysiol 2007; 18: pp. 169-173.
24. Ren J.F., Lin D., Marchlinski F.E., et. al.: Esophageal imaging and strategies for avoiding injury during left atrial ablation for atrial fibrillation. Heart Rhythm 2006; 3: pp. 1156-1161.
25. Orlov M.V., Hoffmeister P., Chaudhry G.M., et. al.: Three-dimensional rotational angiography of the left atrium and esophagus—a virtual computed tomography scan in the electrophysiology lab?. Heart Rhythm 2007; 4: pp. 37-43.
26. Thiagalingam A., Manzke R., D’Avila A., et. al.: Intraprocedural volume imaging of the left atrium and pulmonary veins with rotational X-ray angiography: implications for catheter ablation of atrial fibrillation. J Cardiovasc Electrophysiol 2008; 19: pp. 293-300.
27. Li J.H., Haim M., Movassaghi B., et. al.: Segmentation and registration of three-dimensional rotational angiogram on live fluoroscopy to guide atrial fibrillation ablation: a new online imaging tool. Heart Rhythm 2009; 6: pp. 231-237.
28. Sherzer A.I., Feigenblum D.Y., Kulkarni S., et. al.: Continuous nonfluoroscopic localization of the esophagus during radiofrequency catheter ablation of atrial fibrillation. J Cardiovasc Electrophysiol 2007; 18: pp. 157-160.
29. Nolker G., Gutleben K.J., Marschang H., et. al.: Three-dimensional left atrial and esophagus reconstruction using cardiac C-arm computed tomography with image integration into fluoroscopic views for ablation of atrial fibrillation: accuracy of a novel modality in comparison to multislice computed tomography. Heart Rhythm 2008; 5: pp. 1651-1657.
30. Piorkowski C., Hindricks G., Schreiber D., et. al.: Electroanatomic reconstruction of the left atrium, pulmonary veins, and esophagus compared with the “true anatomy” on multislice computed tomography in patients undergoing catheter ablation of atrial fibrillation. Heart Rhythm 2006; 3: pp. 317-327.
31. Redfearn D.P., Trim G.M., Skanes A.C., et. al.: Esophageal temperature monitoring during radiofrequency ablation of atrial fibrillation. J Cardiovasc Electrophysiol 2005; 16: pp. 589-593.
32. Cummings J.E., Barrett C.D., Litwak K.N., et. al.: Esophageal luminal temperature measurement underestimates esophageal tissue temperature during radiofrequency ablation within the canine left atrium: comparison between 8 mm tip and open irrigation catheters. J Cardiovasc Electrophysiol 2008; 19: pp. 641-644.
33. Kennedy R., Good E., Oral H., et. al.: Temporal stability of the location of the esophagus in patients undergoing a repeat left atrial ablation procedure for atrial fibrillation or flutter. J Cardiovasc Electrophysiol 2008; 19: pp. 351-355.