
Rationale and Objectives
Application of a previously developed model-based algorithm on hyperpolarized (HP) 3 He magnetic resonance (MR) dynamic projection images of phantoms was extended to investigate the utility of HP 3 He MR imaging (MRI) in quantifying airway caliber changes associated with asthma.
Materials and Methods
Airways of seven volunteers were imaged and measured using HP 3 He MRI and multidetector-row computed tomography (MDCT) before and after a methacholine (MCh) challenge. MDCT data were obtained at functional residual capacity and 1 L above functional residual capacity.
Results
Comparison of the resultant data showed that HP 3 He MRI did not match MDCT in measuring the ratios of airway calibers before and after the MCh challenge in 37% to 43% of the airways from the first six generations at the two lung volumes tested. However, MDCT did yield the observation that 49% to 69% of these airways displayed bronchodilation following MCh challenge.
Conclusion
The current implementation of HP 3 He MRI did not match the MCh-induced postchallenge-to-prechallenge airway caliber ratios as measured with MDCT. Elevated parenchymal tethering due to bronchoconstriction-induced hyperinflation was proposed as a possible explanation for this airway dilation.
High-resolution computed tomography (HRCT) has been the imaging modality of choice for assessing airways in asthma studies ( ). Numerous algorithms have been developed to process the acquired computed tomographic data ( ). Sophisticated software has been successfully developed for the visualization and three-dimensional (3D) rendering of the airway tree ( ). However, the use of ionizing radiation makes computed tomography (CT) undesirable in the event that repeated imaging is necessary to follow the progress of disease.
Hyperpolarized (HP) 3 He magnetic resonance imaging (MRI) has been used to visualize ventilation distribution in both animals ( ) and humans ( ) during breathhold of HP 3 He. HP 3 He MRI has also been used to visualize the airways by acquiring the MR images as the gas travels down the respiratory airway tree of both animals ( ) and humans ( ). HP 3 He MRI was able to observe correlations between ventilation dropouts and airways with low MR signal in broncho-challenged human subjects. Whether HP 3 He MRI could be an effective tool in evaluating airway constriction/dilation in asthmatics has become a subject of interest ( ).
Get Radiology Tree app to read full this article<
Methods
Subject Enrollment
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
MRI Hardware and Imaging
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Computed Tomography Hardware and Imaging
Get Radiology Tree app to read full this article<
Protocol
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 1
Maximum Methacholine Dose Administered to Each Subject During Imaging Experiments
Subject Methacholine dose (mg/ml) Hyperpolarized 3 He Magnetic Resonance Imaging Multidetector-row Computed Tomography HEAL3 25.0 25.0 HEAL4 25.0 25.0 ASTH1 10.0 5.0 ASTH 8 0.3125 0.156 ASTH 13 0.3125 5.0 ASTH 16 5.0 25.0 ASTH 21 25.0 25.0
HEAL, healthy; ASTH, asthmatic.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Image Postprocessing
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<

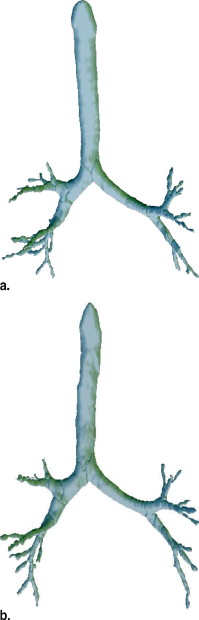
Table 2
Signal-to-Noise Ratio in the Trachea and Main Bronchi from Selected Hyperpolarized 3 He Magnetic Resonance Image Before and After Bronchial Challenge
Subject Tracheal SNR Main Bronchi SNR ⁎ Pre-MCh Post-MCh Pre-MCh Post-MCh HEAL3 67.7 89.7 70.9 71.9 HEAL4 120.8 108.1 75.1 62.4 ASTH1 133.4 97.1 79.7 38.5 ASTH 8 114.3 113.7 72.3 39.7 ASTH 13 98.4 92.2 75.4 67.8 ASTH 16 86.9 59.5 51.5 36.9 ASTH 21 107.8 94.7 90.7 63.8
MCh, methacholine; SNR, signal-to-noise ratio; HEAL, healthy; ASTH, asthmatic.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 3
Number of Airways Visible and Their Response as Observed Through Multidetector-Row Computed Tomography
Airway Generation Airways Visible with Both Imaging Modalities ⁎ CT Measurements Available Both at Pre-MCh and Post-MCh † CT Measurements Indicate Airway Dilation Due to Bronchial Challenge † FRC FRC+1L FRC FRC+1L Trachea 7 7 7 6 6 First 14 14 14 13 14 Second 21 21 21 16 19 Third 43 34 42 17 27 Fourth 26 16 20 7 13 Fifth 16 5 14 3 9 Sum 127 97 118 62 88
CT, computed tomography; FRC, functional residual capacity; 1L, 1 liter; MCh, methacholine; MDCT, multidetector-row computed tomography.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Measurement Accuracy
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Potential Experimental Sources of Difference Between MRI and MDCT Measurements
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Pathophysiological Implications
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Conclusion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Amirav I., Kramer S.S., Grunstein M.M., et. al.: Assessment of methacholine-induced airway constriction by ultrafast high-resolution computed tomography. J Appl Physiol 1993; 75: pp. 2239-2250.
2. Awadh N., Muller N.L., Park C.S., et. al.: Airway wall thickness in patients with near fatal asthma and control groups: Assessment with high resolution computed tomographic scanning. Thorax 1998; 53: pp. 248-253.
3. King G.G., Muller N.L., Whittall K.P., et. al.: An analysis algorithm for measuring airway lumen and wall areas from high-resolution computed tomographic data. Am J Respir Crit Care Med 2000; 161: pp. 574-580.
4. Brown R.H., Croisille P., Mudge B., et. al.: Airway narrowing in healthy humans inhaling methacholine without deep inspiration demonstrated by HRCT. Am J Respir Crit Care Med 2000; 161: pp. 1256-1263.
5. Little S.A., Sproule M.W., Cowan M.D., et. al.: High resolution computed tomographic assessment of airway wall thickness in chronic asthma: Reproducibility and relationship with lung function and severity. Thorax 2002; 57: pp. 247-253.
6. Aykac D., Hoffman E.A.: Segmentation and analysis of the human airway tree from three-dimensional X-ray CT images. IEEE Trans Med Imag 2003; 22: pp. 940-950.
7. Nakano Y., Muro S., Sakai H., et. al.: Computed tomographic measurements of airway dimensions and emphysema in smokers. Am J Respir Crit Care Med 2000; 162: pp. 1102-1108.
8. Brown M.S., McNitt-Gray M.F., Mankovich N.J., et. al.: Method for segmenting chest CT image data using an anatomical model: preliminary results. IEEE Trans Med Imag 1997; 16: pp. 828-839.
9. Kiraly A.P., Higgins W.E., McLennan G., et. al.: Three-dimensional human airway segmentation methods for clinical virtual bronchoscopy. Acad Radiol 2002; 9: pp. 1153-1168.
10. Wood S.A., Zerhouni E.A., Hoford J.D., et. al.: Measurement of three-dimensional lung tree structures by using computed tomography. J Appl Physiol 1995; 79: pp. 1687-1697.
11. Tschirren J., Hoffman E.A., McLennan G., et. al.: Intrathoracic airway trees: Segmentation and airway morphology from low dose CT scans. IEEE Trans Med Imag 2005; 24: pp. 1529-1539.
12. Tschirren J., McLennan G., Palagyi K., et. al.: Matching and anatomical labeling of human airway tree. IEEE Trans Med Imag 2005; 24: pp. 1540-1547.
13. Viallon M., Berthezene Y., Decorps M., et. al.: Laser-polarized 3He as a probe for dynamic regional measurements of lung perfusion and ventilation using magnetic resonance imaging. Magn Reson Med 2000; 44: pp. 1-4.
14. Dupuich D., Berthezene Y., Clouet P.-L., et. al.: Dynamic 3He imaging for quantification of regional lung ventilation parameters. Magn Reson Med 2003; 50: pp. 777-783.
15. Viallon M., Berthezene Y., Callot V., et. al.: Dynamic imaging of hyperpolarized 3He distribution in rat lungs using interleaved-spiral scans. NMR Biomed 2000; 13: pp. 207-213.
16. MacFall J.R., Charles H.C., Black R.D., et. al.: Human lung air spaces: Potential for MR imaging with hyperpolarized He-3. Radiology 1996; 200: pp. 553-558.
17. Guenther D., Eberle B., Hast J., et. al.: 3He MRI in healthy volunteers: Preliminary correlation with smoking history and lung volumes. NMR Biomed 2000; 13: pp. 182-189.
18. Kauczor H.-U., Hofmann D., Kreitner K.-F., et. al.: Normal and abnormal pulmonary ventilation: Visualization at hyperpolarized He-3 MR imaging. Radiology 1996; 201: pp. 564-568.
19. Moller H.E., Chen X.J., Chawla M.S., et. al.: Sensitivity and resolution in 3D NMR microscopy of the lung with hyperpolarized noble gases. Magn Reson Med 1999; 41: pp. 800-808.
20. Chen B.T., Brau A.C.S., Johnson G.A., et. al.: Measurement of regional lung function in rats using hyperpolarized 3Helium dynamic MRI. Magn Reson Med 2003; 49: pp. 78-88.
21. Moller H.E., Chen X.J., Chawla M.S., et. al.: Signal dynamics in magnetic resonance imaging of the lung with hyperpolarized noble gases. J Magn Reson 1998; 135: pp. 133-143.
22. Chen X.J., Chawla M.S., Hedlund L.W., et. al.: MR microscopy of lung airways with hyperpolarized 3He. Magn Reson Med 1998; 39: pp. 79-84.
23. Salerno M., Altes T.A., Brookeman J.R., et. al.: Dynamic spiral MRI of pulmonary gas flow using hyperpolarized 3He: Preliminary studies in healthy and diseased lungs. Magn Reson Med 2001; 46: pp. 667-677.
24. Wild J.M., Paley M.N.J., Kasuboski L., et. al.: Dynamic radial projection MRI of inhaled hyperpolarized 3He gas. Magn Reson Med 2003; 49: pp. 991-997.
25. Tooker A.C., Hong K.S., McKinstry E.L., et. al.: Distal airways in humans: dynamic hyperpolarized 3He MR imaging—Feasibility. Radiology 2003; 227: pp. 575-579.
26. Lewis T.A., Tzeng Y.S., McKinstry E.L., et. al.: Quantification of airway diameters and 3D airway tree rendering from dynamic hyperpolarized 3He magnetic resonance imaging. Magn Reson Med 2005; 53: pp. 474-478.
27. Tzeng Y.S., Mansour J., Handler Z., et. al.: Measurement of the internal diameter of plastic tubes from projection MR images using a model-based least-squares fit approach. Med Phys 2006; 33: pp. 1643-1653.
28. Tzeng Y.S., Hoffman E.A., Cook-Granroth J., et. al.: Comparison of airway diameter measurements from an anthropomorphic airway tree phantom using hyperpolarized 3 He MRI and high-resolution computed tomography. Magn Reson Med 2007; 58: pp. 636-642.
29. King G.G., Carroll J.D., Muller N.L., et. al.: Heterogeneity of narrowing in normal and asthmatic airways measured by HRCT. Eur Respir J 2004; 24: pp. 211-218.
30. Brown R.H., Scichilone N., Mudge B., et. al.: High-resolution computed tomographic evaluation of airway distensibility and the effects of lung inflation on airway caliber in healthy subjects and individuals with asthma. Am J Respir Crit Care Med 2001; 163: pp. 994-1001.
31. Goldin J.G., McNitt-Gray M.F., Sorenson S.M., et. al.: Airway hyperreactivity: Assessment with helical thin-section CT. Radiology 1998; 208: pp. 321-329.
32. Mitzner W., Brown R.H.: Potential mechanism of hyperresponsive airways. Am J Respir Crit Care Med 2000; 161: pp. 1619-1623.
33. National Institutes of Health, National Heart, Lung, and Blood Institute: Guidelines for the Diagnosis and Management of Asthma.1997.NIHBethesda, MD
34. Society A.T.: Guidelines for Methacholine and exercise challenge testing—1999. Am J Respir Crit Care Med 2000; 161: pp. 309-329.
35. Happer W., Miron E., Schaefer S., et. al.: Polarization of the nuclear spins of noble gas atoms by spin exchange with optically pumped alkali metal atoms. Phys Rev 1984; 29: pp. 3092-3110.
36. Brusasco V., Crimi E., Barisione G., et. al.: Airway responsiveness to methacholine: Effects of deep inhalations and airway inflammation. J Appl Physiol 1999; 87: pp. 567-573.
37. Skloot G., Permutt S., Togias A., et. al.: Airway hyperresponsiveness in asthma: A problem of limited smooth muscle relaxation with inspiration. J Clin Invest 1995; 96: pp. 2393-2403.
38. Reinhardt J.M., D’Souza N.D., Hoffman E.A., et. al.: Accurate measurement of intrathoracic airways. IEEE Trans Med Imag 1997; 16: pp. 820-827.
39. Verbanck S., Schuermans D., Noppen M., et. al.: Evidence of acinar airway involvement in asthma. Am J Respir Crit Care Med 1999; 159: pp. 1545-1550.
40. Verbanck S., Schuermans D., Van Muylem A., et. al.: Ventilation distribution during histamine provocation. J Appl Physiol 1997; 83: pp. 1907-1916.
41. Verbanck S., Schuermans D., Paiva M., et. al.: Nonreversible conductive airway ventilation heterogeneity in mild asthma. J Appl Physiol 2003; 94: pp. 1380-1386.
42. Hansell D.M.: Small airways diseases: Detection and insights with computed tomography. Eur Respir J 2001; 17: pp. 1294-1313.
43. Altes T.A., Powers P.L., Knight-Scott J., et. al.: Hyperpolarized 3He MR lung ventilation imaging in asthmatics: Preliminary findings. J Magn Res Imag 2001; 13: pp. 378-384.
44. Holmes JH, O’Halloran RL, Brodsky EK, et al. Imaging 3D respiratory dynamics using hyperpolarized He-3 multi-echo HYPR VIPR, in Proceedings of the International Society of Magnetic Resonance in Medicine. Berlin, Germany, May 19–25, 2007.
45. Peterson ET, Holmes JH, Gonzalez-Fernandez G, et al. Details on the 3D airway segmentation algorithm using the 3D PR data, in Proceedings of the International Society of Magnetic Resonance in Medicine. Berlin, Germany, May 19–25, 2007.
46. Han B.K., Im J.G., Kim H.S., et. al.: Airway reactivity to bronchoconstrictor and bronchodilator: Assessment using thin-section and volumetric three-dimensional CT. Korean J Radiol 2000; 1: pp. 127-134.
47. Nagase T., Moretto A., Ludwig M.S., et. al.: Airway and tissue behavior during induced constriction in rats: Intravenous vs. aerosol administration. J Appl Physiol 1994; 76: pp. 830-838.
48. Petak F., Hantos Z., Adamicza A., et. al.: Methacholine-induced bronchoconstriction in rats: Effects of intravenous vs. aerosol delivery. J Appl Physiol 1997; 82: pp. 1479-1487.