
Rationale and Objectives
We sought to evaluate the effectiveness of e-mail communication to reduce the utilization of computed tomography for pulmonary thromboembolism (PE) in young patients (aged 40 and under) in our institution.
Materials and Methods
An e-mail was sent to all of our institution’s emergency department (ED) physicians in response to a series of negative PE studies in young females. The periods 90 days before and 90 days after were evaluated to assess the total number of PE studies performed in patients aged 40 and younger, the rate of positivity, and the utilization of D-dimer and ventilation/perfusion scans during each period.
Results
Over the 180-day period, a total of 65 PE studies were ordered in patients aged 40 and younger in the ED. Studies were positive for PE in 1 of 33 (3%) before the e-mail and 4 of 32 (12.5%) after ( P = .343). There was no difference in the number of D-dimer studies ordered during each period for patients studied with computed tomography. Ventilation/perfusion scanning was not performed on any ED patients younger than 40 during the 180-day period.
Conclusions
One-time e-mail communication was not effective in changing ED ordering habits of PE studies. Scant information exists in regard to effective clinician-to-clinician communication. Further evaluation for successful mechanisms to promote health practice reform and quality improvement is necessary.
With an estimated annual incidence rate of 0.1% ( ), approximately 300,000 people in the United States are expected to be diagnosed with pulmonary embolism (PE) each year. If PE is recognized and treated, mortality is relatively low; however, a multicenter trial found all-cause mortality for patients with PE to be 17% at 3 months ( ). Thus, PE accounts for roughly 50,000 deaths in the United States per year.
Computed tomographic (CT) pulmonary angiography (CTPA) has become the diagnostic test of choice for PE owing to its high negative predictive value ( ). This success is a double-edge sword—as techniques improve and availability increases, ordering patterns have shifted to a greater reliance on CTPA even in those patients with a low pretest probability. In the Prospective Investigation of Pulmonary Embolism Diagnosis (PIOPED I) study, the positive rate of patients who underwent evaluation for pulmonary embolus was 33% ( ). The positive rate for patients undergoing CTPA appears to be decreasing and in one institution dropped from 27% to 16% over a 5-year period ( ). In the emergency department (ED), positivity rates may be even lower, with one study showing a CTPA positivity rate of 13.7% even after excluding low-risk subjects ( ). Positive rates range from 8% to 14% in our institution depending on the ordering service and remain between 10% and 12% for the ED (unpublished data from periodic quality assurance review).
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Materials And Methods
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
“The number of PE studies from the ED has been trending upwards, in some cases five in one night. It may well be that all are justifiable and indicated, but I fear that it may become the de facto chest radiograph. The doses of a CT PE study confer between a 5–15% increase in the risk of development of breast cancer in women under the age of 35. In young women with a negative chest radiograph, I would ask that ordering a V/Q scan be considered.”
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
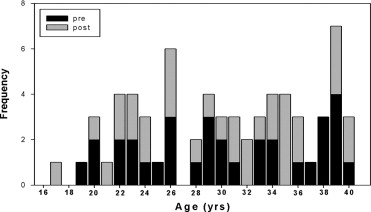
Table 1
Comparison of Pre−E-mail and Post−E-mail Correspondence for CT Positivity, D-dimer Ordering, and V̇/Q̇ Scans Performed
Pre−E-mail ( n = 33) Post−E-mail ( n = 32)P -value CT positivity 1/33 (3.03%) 4/32 (12.5%) .34 D-dimer ordered 13/33 (39.4%) 15/32 (46.9%) .98 D-dimer Positive 9/13 (69.2%) 11/13 (84.6%) .74 V̇/Q̇ scan performed 0/33 0/32 1.00
Values are given as frequency (%). All P values are derived from the χ 2 /Fisher’s test.
\* P < .05.
Table 2
Common Indications and Predisposing Conditions for PE Studies
Condition Pre−E-mail Post−E-mail Chest pain 19 20 Shortness of breath 21 17 Tachycardia 6 1 Postpartum 2 7 Malignancy 4 1 Prior PE, DVT, or DVT symptoms 9 4
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Conclusion
Get Radiology Tree app to read full this article<
References
1. Ageno W., Squizzato A., Garcia D., Imberti D.: Epidemiology and risk factors of venous thromboembolism. Semin Thromb Hemost 2006; 32: pp. 651-658.
2. Goldhaber S.Z., Visani L., De Rosa M.: Acute pulmonary embolism: Clinical outcomes in the International Cooperative Pulmonary Embolism Registry (ICOPER). Lancet 1999; 353: pp. 1386-1389.
3. Quiroz R., Kucher N., Zou K.H., et. al.: Clinical validity of a negative computed tomography scan in patients with suspected pulmonary embolism: A systematic review. JAMA 2005; 293: pp. 2012-2017.
4. The PIOPED Investigators: Value of the ventilation/perfusion scan in acute pulmonary embolism. JAMA 1990; 263: pp. 2753-2759.
5. Prologo J.D., Glauser J.: Variable diagnostic approach to suspected pulmonary embolism in the ED of a major academic tertiary care center. Am J Emerg Med 2002; 20: pp. 5-9.
6. Anderson D.R., Kovacs M.J., Dennie C., et. al.: Use of spiral computed tomography contrast angiography and ultrasonography to exclude the diagnosis of pulmonary embolism in the emergency department. J Emerg Med 2005; 29: pp. 399-404.
7. Hurwitz L.M., Reiman R.E., Yoshizumi T.T., et. al.: Radiation dose from contemporary cardiothoracic multidetector CT protocols with an anthropomorphic female phantom: Implications for cancer induction. Radiology 2007; 245: pp. 742-750.
8. Stein P.D., Woodard P.K., Weg J.G., et. al.: Diagnostic pathways in acute pulmonary embolism: Recommendations of the PIOPED II Investigators. Radiology 2007; 242: pp. 15-21.
9. Hurwitz L.M., Yoshizumi T.T., Reiman R.E., et. al.: Radiation dose to the female breast from 16-MDCT body protocols. AJR Am J Roentgenol 2006; 186: pp. 1718-1722.
10. Lee C.I., Haims A.H., Monico E.P., Brink J.A., Forman H.P.: Diagnostic CT scans: Assessment of patient, physician, and radiologist awareness of radiation dose and possible risks. Radiology 2004; 231: pp. 393-398.
11. Cushman M.: Epidemiology and risk factors for venous thrombosis. Semin Hematol 2007; 44: pp. 62-69.
12. Cook J.V., Kyriou J.: Radiation from CT and perfusion scanning in pregnancy. BMJ 2005; 331: pp. 350.
13. Remy-Jardin M., Pistolesi M., Goodman L.R., et. al.: Management of suspected acute pulmonary embolism in the era of CT angiography: A statement from the Fleischner Society. Radiology 2007; 245: pp. 315-329.
14. Kearon C., Ginsberg J.S., Douketis J., et. al.: An evaluation of D-dimer in the diagnosis of pulmonary embolism: A randomized trial. Ann Intern Med 2006; 144: pp. 812-821.
15. Stone E., Roach P., Bernard E., et. al.: Use of computed tomography pulmonary angiography in the diagnosis of pulmonary embolism in patients with an intermediate probability ventilation/perfusion scan. Intern Med J 2003; 33: pp. 74-78.
16. Coiera E., Tombs V.: Communication behaviours in a hospital setting: An observational study. BMJ 1998; 316: pp. 673-676.
17. Murtaugh C.M., Pezzin L.E., McDonald M.V., Feldman P.H., Peng T.R.: Just-in-time evidence-based e-mail “reminders” in home health care: Impact on nurse practices. Health Serv Res 2005; 40: pp. 849-864.
18. Feldman P.H., Murtaugh C.M., Pezzin L.E., McDonald M.V., Peng T.R.: Just-in-time evidence-based e-mail “reminders” in home health care: Impact on patient outcomes. Health Serv Res 2005; 40: pp. 865-885.
19. Tierney W.M., Overhage J.M., Murray M.D., et. al.: Can computer-generated evidence-based care suggestions enhance evidence-based management of asthma and chronic obstructive pulmonary disease?. Health Serv Res 2005; 40: pp. 477-497.
20. Sequist T.D., Gandhi T.K., Karson A.S., et. al.: A randomized trial of electronic clinical reminders to improve quality of care for diabetes and coronary artery disease. J Am Med Inform Assoc 2005; 12: pp. 431-437.
21. Tierney W.M., Overhage J.M., Murray M.D., et. al.: Effects of computerized guidelines for managing heart disease in primary care. J Gen Intern Med 2003; 18: pp. 967-976.
22. Kerry S., Oakeshott P., Dundas D., Williams J.: Influence of postal distribution of the Royal College of Radiologists’ guidelines, together with feedback on radiological referral rates, on x-ray referrals from general practice: A randomized controlled trial. Fam Pract 2000; 17: pp. 46-52.
23. Freeborn D.K., Shye D., Mullooly J.P., Eraker S., Romeo J.: Primary care physicians’ use of lumbar spine imaging tests: Effects of guidelines and practice pattern feedback. J Gen Intern Med 1997; 12: pp. 619-625.
24. Rosenthal D.I., Weilburg J.B., Schultz T., et. al.: Radiology order entry with decision support: Initial clinical experience. J Am Coll Radiol 2006; 3: pp. 799-806.
25. Amis E.S., Butler P.F., Applegate K.E., et. al.: American College of Radiology white paper on radiation dose in medicine. J Am Coll Radiol 2007; 4: pp. 272-284.
26. Wells P.S., Anderson D.R., Rodger M., et. al.: Derivation of a simple clinical model to categorize patients probability of pulmonary embolism: Increasing the models utility with the SimpliRED D-dimer. Thromb Haemost 2000; 83: pp. 416-420.
27. Kline J.A., Mitchell A.M., Kabrhel C., Richman P.B., Courtney D.M.: Clinical criteria to prevent unnecessary diagnostic testing in emergency department patients with suspected pulmonary embolism. J Thromb Haemost 2004; 2: pp. 1247-1255.