
Rationale and Objectives
To evaluate prospectively, in patients with suspected or known urinary stone disease, the image quality and diagnostic confidence of nonenhanced abdominal low-dose computed tomography (CT) with iterative reconstruction (IR) compared to filtered back-projection (FBP).
Materials and Methods
Fifty consecutive patients with suspected ( n = 33) or known ( n = 17) urinary stone disease underwent nonenhanced abdominal low-dose CT (120 kVp, 30 effective mAs, 1.6 ± 0.5 mSv). Reconstructions were performed with sinogram-affirmed IR and with FBP. Attenuation (in Hounsfield units) was measured in subcutaneous fat and urinary bladder; image noise was determined. Two readers assessed image quality, number and location of urinary calculi were recorded, and diagnostic confidence was assessed. Statistical analyses included Mann-Whitney, Friedman’s two-way, Wilcoxon signed rank, Pearson’s, and Spearman’s rank order correction tests.
Results
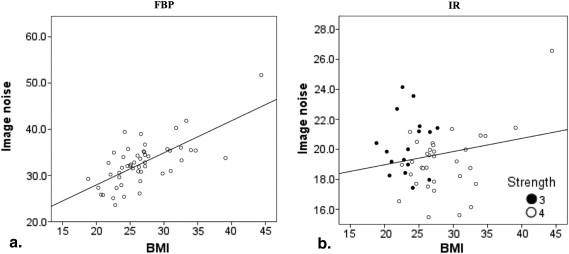
Attenuation of urinary bladder ( P = .208, reader 1; P = .123, reader 2) and fat ( P = .568, reader 1; P = .834, reader 2) was similar among FBP and IR datasets. Image noise was reduced in IR datasets by 40.1% ( P < .001). IR improved image quality ( P < .01), and obesity as factor impairing image quality was noted in FBP but not in IR images ( P < .05). There was no significant difference in number of calculi in datasets reconstructed with IR and FBP ( P = .102, reader 1; P = .059, reader 2). Diagnostic confidence regarding identification of urinary calculi improved with IR ( P < .05, reader 1; P < .01, reader 2).
Conclusion
IR improves image quality and confidence for diagnosing urinary stone disease in abdominal low-dose CT.
Nonenhanced abdominal computed tomography (CT) is considered the reference standard imaging technique in patients with suspected or known urinary stone disease . This is due to the superiority of nonenhanced abdominal CT compared to abdominal plain film radiography in regard to the sensitivity and specificity for the diagnosis of urinary stones . The downside of abdominal CT compared to plain film radiography, however, is the higher radiation dose of the technique. This has triggered various strategies for radiation dose reduction, such as noise reduction filters or low tube current scanning .
By doing so, some studies could demonstrate that nonenhanced low radiation dose abdominal CT may be an appropriate imaging tool for the diagnosis of urinary stone disease . However, other studies reported limited diagnostic capabilities of low-radiation-dose abdominal CT, mainly due to increased noise leading to reduced confidence . It is likely that these concerns have precluded the wide application of low-radiation-dose abdominal CT protocols as the standard initial imaging test in patients with urinary stone disease .
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Materials and methods
Patient Population
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
CT Protocol
Get Radiology Tree app to read full this article<
CT Data Reconstruction
Get Radiology Tree app to read full this article<

Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
CT Data Analysis
Get Radiology Tree app to read full this article<
Quantitative analysis
Get Radiology Tree app to read full this article<
Image noise
Get Radiology Tree app to read full this article<
Image quality
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Urinary stone disease
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Table 1
Patient Demographics
Total No. of patients 50 Female 12 Age (years) 50.3 ± 17.4 (18–88) Height (m) 1.7 ± 0.1 (1.55–1.87) Weight (kg) 80.4 ± 13.6 (48–98) Body mass index (kg/m 2 ) 26.8 ± 4.8 (18.8–34.7)
Values are mean ± standard deviation with range in parentheses.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Quantitative Assessment
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
![Figure 2, Comparison of computed tomography attenuation values (in Hounsfield units [HU]) in datasets reconstructed with filtered back-projection (FBP) and iterative reconstruction (IR) at strength levels from 1 to 5 showing similar values in the urinary bladder (a) ( P = .208, reader 1; P = .123, reader 2) and subcutaneous fat (b) ( P = .568, reader 1; P = .834, reader 2). (c) Noise was significantly reduced with IR ( P < .001). In FBP images, noise was lower in patients with a body mass index (BMI) <30 kg/m 2 compared to patients with a BMI ≥30 kg/m 2 ( P < .001), while there was no such difference in patients with IR ( P = .806).](https://storage.googleapis.com/dl.dentistrykey.com/clinical/IterativeReconstructionsversusFilteredBackProjectionforUrinaryStoneDetectioninLowDoseCT/1_1s20S1076633213003899.jpg)
Get Radiology Tree app to read full this article<
Image Noise
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Image Quality
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 2
Image Quality and Image Quality–Reducing Factors Among Datasets Reconstructed with Filtered Back-Projection (FBP) and Iterative Reconstruction (IR)
FBP IR_P_ -Value Image quality Kidney Median (range) 3 (2–4) 3 (2–4) .001 Mean 3.24 2.96 Ureter Median (range) 3 (3–5) 3 (2–5) .001 Mean 3.40 3.18 Urinary bladder Median (range) 3 (3–5) 3 (3–4) .763 Mean 3.40 3.38 Image quality–reducing factors Obesity Median (range) 3 (2–4) 3 (2–4) <.05 Mean 2.94 2.76
Image quality: score 1, excellent; score 2, above average; score 3, acceptable; score 4, substandard; score 5, not acceptable. Image quality-reducing factors: Score 1, no artifacts; score 2, minor artifacts not affecting the visualization of any structure; score 3, major artifacts affecting the visualization of any structure; score 4, affecting diagnostic information.
Get Radiology Tree app to read full this article<
Urinary Stone Disease
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Smith R.C., Rosenfield A.T., Choe K.A., et. al.: Acute flank pain: comparison of non-contrast-enhanced CT and intravenous urography. Radiology 1995; 194: pp. 789-794.
2. Boulay I., Holtz P., Foley W.D., et. al.: Ureteral calculi: diagnostic efficacy of helical CT and implications for treatment of patients. AJR Am J Roentgenol 1999; 172: pp. 1485-1490.
3. Vieweg J., Teh C., Freed K., et. al.: Unenhanced helical computerized tomography for the evaluation of patients with acute flank pain. J Urol 1998; 160: pp. 679-684.
4. Abramson S., Walders N., Applegate K.E., et. al.: Impact in the emergency department of unenhanced CT on diagnostic confidence and therapeutic efficacy in patients with suspected renal colic: a prospective survey. 2000 ARRS President’s Award. American Roentgen Ray Society. AJR Am J Roentgenol 2000; 175: pp. 1689-1695.
5. Eray O., Cubuk M.S., Oktay C., et. al.: The efficacy of urinalysis, plain films, and spiral CT in ED patients with suspected renal colic. Am J Emerg Med 2003; 21: pp. 152-154.
6. Hamm M., Wawroschek F., Weckermann D., et. al.: Unenhanced helical computed tomography in the evaluation of acute flank pain. Eur Urol 2001; 39: pp. 460-465.
7. Kalra M.K., Maher M.M., Blake M.A., et. al.: Detection and characterization of lesions on low-radiation-dose abdominal CT images postprocessed with noise reduction filters. Radiology 2004; 232: pp. 791-797.
8. Poletti P.A., Platon A., Rutschmann O.T., et. al.: Low-dose versus standard-dose CT protocol in patients with clinically suspected renal colic. AJR Am J Roentgenol 2007; 188: pp. 927-933.
9. Dougeni E., Faulkner K., Panayiotakis G.: A review of patient dose and optimisation methods in adult and paediatric CT scanning. Eur J Radiol 2012; 81: pp. e665-e683.
10. Tack D., Sourtzis S., Delpierre I., et. al.: Low-dose unenhanced multidetector CT of patients with suspected renal colic. AJR Am J Roentgenol 2003; 180: pp. 305-311.
11. Niemann T., Kollmann T., Bongartz G.: Diagnostic performance of low-dose CT for the detection of urolithiasis: a meta-analysis. AJR Am J Roentgenol 2008; 191: pp. 396-401.
12. Hamm M., Knopfle E., Wartenberg S., et. al.: Low dose unenhanced helical computerized tomography for the evaluation of acute flank pain. J Urol 2002; 167: pp. 1687-1691.
13. Katz D.S., Venkatarmanan N., Napel S., et. al.: Can low-dose unenhanced multidetector CT be used for routine evaluation of suspected renal colic?. AJR Am J Roentgenol 2003; 180: pp. 113-115.
14. Katz D.S., Scheer M., Lumerman J.H., et. al.: Alternative or additional diagnoses on unenhanced helical computed tomography for suspected renal colic: experience with 1000 consecutive examinations. Urology 2000; 56: pp. 53-57.
15. Funama Y., Oda S., Utsunomiya D., et. al.: Coronary artery stent evaluation by combining iterative reconstruction and high-resolution kernel at coronary CT angiography. Acad Radiol 2012; 19: pp. 1324-1331.
16. Pontana F., Pagniez J., Flohr T., et. al.: Chest computed tomography using iterative reconstruction vs filtered back projection (Part 1): evaluation of image noise reduction in 32 patients. Eur Radiol 2011; 21: pp. 627-635.
17. Baumueller S., Winklehner A., Karlo C., et. al.: Low-dose CT of the lung: potential value of iterative reconstructions. Eur Radiol 2012; 22: pp. 2597-2606.
18. Kulkarni N.M., Uppot R.N., Eisner B.H., et. al.: Radiation dose reduction at multidetector CT with adaptive statistical iterative reconstruction for evaluation of urolithiasis: how low can we go?. Radiology 2012; 265: pp. 158-166.
19. Sagara Y., Hara A.K., Pavlicek W., et. al.: comparison of low-dose CT with adaptive statistical iterative reconstruction and routine-dose CT with filtered back projection in 53 patients. AJR Am J Roentgenol 2010; 195: pp. 713-719.
20. Takx R.A., Schoepf U.J., Moscariello A., et. al.: Coronary CT angiography: comparison of a novel iterative reconstruction with filtered back projection for reconstruction of low-dose CT-Initial experience. Eur J Radiol 2013; 82: pp. 275-280.
21. Wang R., Schoepf U.J., Wu R., et. al.: Image quality and radiation dose of low dose coronary CT angiography in obese patients: sinogram affirmed iterative reconstruction versus filtered back projection. Eur J Radiol 2012; 81: pp. 3141-3145.
22. Yanagawa M., Honda O., Yoshida S., et. al.: Adaptive statistical iterative reconstruction technique for pulmonary CT: image quality of the cadaveric lung on standard- and reduced-dose CT. Acad Radiol 2010; 17: pp. 1259-1266.
23. American Association of Physicists in Medicine Task Group 23 : The measurement, reporting, and management of radiation dose in CT.2008.American Association of Physicists in Medicine Task Group 23College Park, MD
24. Kalra M.K., Maher M.M., Sahani D.V., et. al.: Low-dose CT of the abdomen: evaluation of image improvement with use of noise reduction filters pilot study. Radiology 2003; 228: pp. 251-256.
25. Prakash P., Kalra M.K., Kambadakone A.K., et. al.: Reducing abdominal CT radiation dose with adaptive statistical iterative reconstruction technique. Invest Radiol 2010; 45: pp. 202-210.
26. Landis J.R., Koch G.G.: The measurement of observer agreement for categorical data. Biometrics 1977; 33: pp. 159-174.
27. Winklehner A., Karlo C., Puippe G., et. al.: Raw data-based iterative reconstruction in body CTA: evaluation of radiation dose saving potential. Eur Radiol 2011; 21: pp. 2521-2526.
28. Korn A., Bender B., Fenchel M., et. al.: Sinogram affirmed iterative reconstruction in head CT: improvement of objective and subjective image quality with concomitant radiation dose reduction. Eur J Radiol 2013 Sep; 82: pp. 1431-1435. Epub 2013 Apr 12