
The lateral chest radiograph is a valuable source of information that has become increasingly undervalued in the era of chest computed tomography. Optimal use of the lateral radiograph requires systematic analysis. First is an overview, followed by analysis of the airway and major hilar structures. Next is attention to the three areas where the image darkens in the absence of visible structure edges. Last is attention to the periphery and the upper abdomen. This communication outlines the systematic analysis and then explains in more detail the value of the critical features of that analysis.
Over the past two or three decades, the lateral chest radiograph has received decreasing attention, both clinically and educationally. Routine chest radiographs, especially of younger adult patients, are often confined to frontal views; laterals are rarely ordered as a follow-up. In modern chest imaging, if the frontal view shows the possibility of an abnormality, many radiologists recommend chest computed tomography (CT). The ability to perform CT has become sufficiently convenient for this to be a practical approach, despite the downsides of chest CT, which include much greater radiation dose than plain radiographs and the high incidence of false-positive findings that may require additional evaluation.
This reasoning has led to less emphasis on the ability of medical trainees, including radiology residents and medical students, to become thoroughly comfortable with the analysis of the lateral radiograph. The problem is compounded by the fact that young radiologists have had all their training during the era since CT became the prime imaging tool for the mediastinum and high-resolution CT became the imaging gold standard for the lungs. This has led many radiologists and other physicians to become less conversant with the details and subtleties of normal and abnormal findings on the lateral radiograph.
Paradoxically and unintentionally, the problem has been compounded by the complexities of the lateral radiograph that have often been taught in the past. The brilliant first generation of chest radiology specialists, especially Benjamin Felson , studied frontal and lateral chest radiographs with such intensity and imagination that they figured out the meaning of each edge and the identity of every structure. They accomplished this without the assistance of cross-sectional imaging of living patients as a reference. With respect to the lateral radiograph, probably the pinnacle of these analyses were the monographs written by Anthony Proto and John Speckman in 1979, in which they described the meaning of each line and edge on the normal lateral radiograph. Learning the lateral radiograph to that level of detail seems less useful in the era of CT.
We thus need to take a new approach to the use of the lateral chest film in the context of modern chest imaging. Although some studies have shown little value to the lateral radiograph in specific instances , most studies and expert opinions continue to show how valuable it is . I believe that the lateral view should be thought of as a full half of the routine chest plain radiographic study. The lateral view often provides key findings that are not visible on the frontal view. It frequently clarifies questionable abnormalities by showing more specific features. It is, in my opinion, the best view to determine lung volumes, because the inflation of the lungs is easier to estimate with the lungs in profile surrounded by the chest wall and hemidiaphragms. It is especially useful in determining whether and why the hilum is abnormal, because the hilar vessels are not overlapped by the mediastinum . Yet a complete search of the lateral radiograph should take less time than that of the frontal radiograph. Understanding the most useful features of the lateral radiograph can be far simpler than many radiologists and other health care professionals have been led to believe.
This communication is intended to outline a systematic approach to the search of the lateral radiograph and the analysis of the most common abnormalities. This approach facilitates familiarity with the normal features and is intended to make the lateral view easier to interpret and to teach to others. The communication consists of two sections: (1) an outline of a systematic search of the lateral radiograph and (2) a more detailed discussion of the two critical features of the search: the hilum and the “three darkenings.” My goal is to make the lateral radiograph more approachable and thus to encourage its continued and increased use, especially by those first being exposed to chest imaging.
Systematic search of the lateral chest radiograph
Get Radiology Tree app to read full this article<
Table 1
Lateral Chest Radiograph Search Pattern
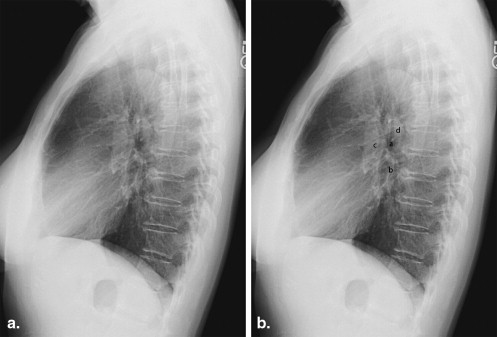
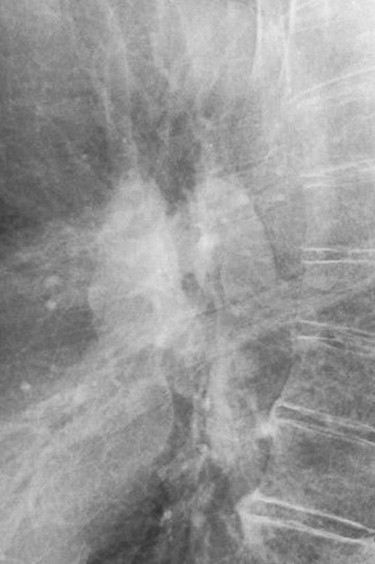
1. Look briefly at the entire image for obvious abnormalities and verify the patient and date information. 2. Judge the size of the lungs and the lung markings and the shape of the diaphragms. 3. Follow the airway from the neck to the hilum. 4. Identify the principal hilar structures: left main bronchus and right and left pulmonary arteries. 5. Look down from the hilum for darkening to the diaphragms. 6. Identify the edge of the left ventricle, then note the darkening from the middle of the heart upward toward the trachea. 7. Cross the trachea and follow the spine down to the diaphragms, judging each vertebral body and looking for darkening until crossing the diaphragms. 8. Evaluate the periphery, beginning with the upper abdominal bowel gas, then the anterior chest wall, lower neck, and posterior ribs, finishing with the costophrenic angles.

Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<

Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Critical features of the lateral search
The Hilum
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<

Get Radiology Tree app to read full this article<
The Three Darkenings
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<


Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<

Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<

Get Radiology Tree app to read full this article<
Conclusions
Get Radiology Tree app to read full this article<
References
1. Felson B.: Chest roentgenology.1973.SaundersPhiladelphia, PA
2. Proto A.V., Speckman J.M.: The left lateral radiograph of the chest. I. Med Radiogr Photogr 1979; 55: pp. 30-74.
3. Proto A.V., Speckman J.M.: The left lateral radiograph of the chest. II. Med Radiogr Photogr 1980; 56: pp. 38-63.
4. Forrest J.V., Sagel S.S.: The lateral radiograph for early diagnosis of lung cancer. Radiology 1979; 131: pp. 309-310.
5. Austin J.H.: The lateral chest radiograph in the assessment of nonpulmonary health and disease. Radiol Clin North Am 1984; 22: pp. 687-698.
6. Dobson M.J., Carrington B.M., Parsons V.J., et. al.: What is the value of the lateral chest radiograph in the follow-up of thoracic lymphoma?. Eur Radiol 1997; 7: pp. 1110-1113.
7. Lynch T., Gouin S., Larson C., et. al.: Does the lateral chest radiograph help pediatric emergency physicians diagnose pneumonia? A randomized clinical trial. Acad Emerg Med 2004; 11: pp. 625-629.
8. Robinson A.E.: The lateral chest radiograph: is it doomed to extinction?. Acad Radiol 1998; 5: pp. 322-323.
9. Thompson B.H., Berbaum K.S., George M.J., et. al.: Identifying left lower lobe pneumonia at chest radiography: performance of family practice residents before and after a didactic session. Acad Radiol 1998; 5: pp. 324-328.
10. McComb B.L.: The chest in profile. J Thorac Imaging 2002; 17: pp. 58-69.