
Rationale and Objectives
To assess whether left atrial (LA) volume, function, and diameter as determined by multidetector computed tomography (MDCT) are associated with the presence and chronicity of atrial fibrillation (AF).
Materials and Methods
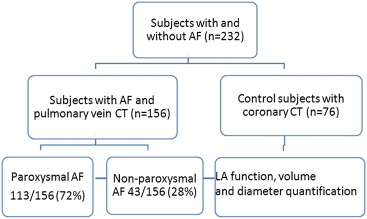
A total of 232 subjects, 156 with AF (43 with chronic and 113 with paroxysmal) and 76 normal subjects, formed the study population. AF subjects underwent MDCT of the pulmonary veins and LA, and normal subjects underwent coronary computed tomography (CT), on which LA volume, function, and diameter were measured. Associations between each MDCT LA parameter and presence and chronicity of AF were assessed using logistic regression analysis.
Results
The indexed LA maximum volume (odds ratio [OR] = 2.42; 95% confidence interval [CI], 1.43–4.08; P = .0009) was significantly associated with chronicity and presence of AF (OR = 1.06; 95% CI, 1.03–1.10; P = .0003) after adjustment for traditional risk factors. The LA function was associated with presence of AF (OR = 0.93; 95% CI, 0.89–0.97; P = .0005), but not with AF chronicity (OR = 1.12; 95% CI, 0.93–1.33; P = .21).
Conclusions
Decreased LA function is associated with presence of AF, and increased LA maximum volume is associated with presence and chronicity of AF, independent of traditional risk factors.
Key points:
Retrospectively gated pulmonary vein and left atrium computed tomography helps clinicians to assess anatomy, volume, and function in patients with atrial fibrillation (AF) before radiofrequency ablation
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Materials and methods
Study Design and Population
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
ECG-Gated Pulmonary Vein and LA MDCT
Get Radiology Tree app to read full this article<
ECG-Gated CCT
Get Radiology Tree app to read full this article<
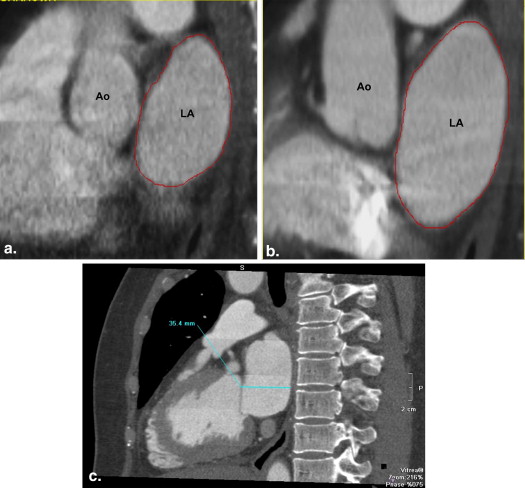
Image Postprocessing
Get Radiology Tree app to read full this article<
LA Function and Volume
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Definitions of MDCT LA Measurements
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Risk Factor and Covariate Assessment
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Results
Study Subjects
Get Radiology Tree app to read full this article<
Table 1
Study Sample Characteristics Presented as Mean ± SD or Median (IQR) when Appropriate
(a) Groups Normal Subjects ( n = 76) Patients with AF ( n = 156)P Value ∗ Age, years 48 (39–58) 59 (52–64) <.0001 † Women, n (%) 37 (48) 45 (29) .003 † Weight, kg 81 (72–91) 95 (81–106) <.0001 † Height, m 1.7 (1.6–1.8) 1.8 (1.7–1.8) .0001 † BMI, kg/m 2 27 (24–31) 28 (26–33) .01 † BSA 1.9 ± 0.2 2.2 ± 0.3 <.0001 † SBP, mm Hg 122 ± 10 123 ± 20 .30 DBP, mm Hg 73 ± 9 75 ± 11 .43 HR, bpm 73 ± 12 78 ± 15 .02 † CAD, n (%) 0 (0) 14 (9) .006 † Hypertension, n (%) 0 (0) 82 (51) <.0001 †
(b) Groups Paroxysmal AF ( n = 113) Chronic AF ( n = 43)P Value ∗ Age, years 58 (51–63) 61, 56-66 .11 Women, n (%) 35 (31) 10 (23) .43 Weight, kg 91 (79–106) 98 (87–111) .01 † Height, m 1.8 (1.7–1.8) 1.8 (1.7–1.9) .12 BMI, kg/m 2 28 (25–32) 30 (27–34) .05 † BSA 2.1 ± 0.3 2.2 ± 0.3 .01 † SBP, mm Hg 121 ± 19 128 ± 21 .06 DBP, mm Hg 72 ± 9 82 ± 11 <.0001 † HR, bpm 77 ± 15 79 ± 15 .56 CAD, n (%) 8 (7) 6 (14) .21 Hypertension, n (%) 50 (44) 32 (74) .001 †
AF, atrial fibrillation; BMI, body mass index; bpm, beats per minute; BSA, body surface area; CAD, coronary artery disease; DBP, diastolic blood pressure; HR, heart rate; SBP, systolic blood pressure; SD, standard deviation.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
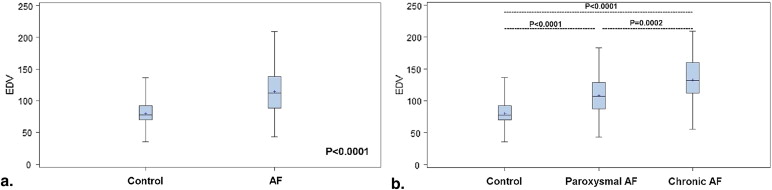
AF and LA Volume and LA Diameter
Get Radiology Tree app to read full this article<
Table 2
Left Atrial Function, Volume, and Diameter (Absolute and Indexed Values) in Normal Patients and Patients with AF (Mean ± SD, 95% Confidence Interval)
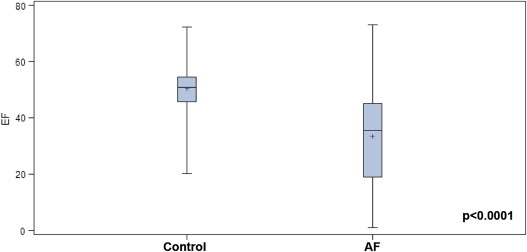
Group Normal AF_P_ Value ∗ N 76 156 Absolute values LA EDV (mL) 80 ± 20 (75–84) 115 ± 33 (110–120) <.0001 † LA ESV (mL) 40 ± 13 (37–43) 79 ± 35 (73–84) <.0001 † LA SV (mL) 40 ± 10 (38–42) 35 ± 18 (32–38) .07 LA EF (%) 50 ± 9 (48–52) 33 ± 16 (30–35) <.0001 † LA diameter (mm) 31 ± 4 (30–32) 41 ± 7 (40–42) <.0001 † Indexed to BSA LA EDV/BSA (mL/m 2 ) 40 ± 9 (38–42) 54 ± 16 (51–56) <.0001 † LA ESV/BSA (mL/m 2 ) 20 ± 6 (19–21) 37 ± 17 (34–40) <.0001 † LA SV/BSA (mL/m 2 ) 20 ± 5 (19–21) 16 ± 8 (15–17) .001 † LA diameter (mm) 16 ± 2 (15–16) 19 ± 3 (18–19) <.0001 †
BSA, body surface area; EDV, end-diastolic volume; EF, ejection fraction; ESV, end-systolic volume; LA, left atrium; STD, standard deviation; SV, stroke volume.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 3
Left Atrial Function, Volume and Diameter (Absolute and Indexed Values) in Paroxysmal and Chronic Atrial Fibrillation (Mean ± SD, 95% Confidence Interval)
Type of Atrial Fibrillation Paroxysmal Chronic_P_ Value ∗ N 113 43 Absolute values LA EDV (mL) 108 ± 29 (102–114) 132 ± 36 (121–143) .0002 † LA ESV (mL) 66 ± 25 (61–71) 112 ± 36 (102–124) <.0001 † LA SV (mL) 42 ± 14 (39–44) 17 ± 14 (13–22) <.0001 † LA EF (%) 39 ± 13 (37–42) 17 ± 13 (13–21) <.0001 † LA diameter (mm) 39 ± 6 (38–40) 46 ± 5 (44–48) <.0001 † Indexed to BSA LA EDV/BSA (mL/m 2 ) 52 ± 14 (49–55) 59 ± 17 (54–65) .01 † LA ESV/BSA (mL/m 2 ) 32 ± 13 (29–34) 51 ± 17 (45–56) <.0001 † LA SV/BSA (mL/m 2 ) 20 ± 6 (18–21) 8 ± 6 (6–10) <.0001 † LA diameter (mm) 19 ± 3 (18–20) 21 ± 3 (20–22) .006 †
BSA, body surface area; EDV, end-diastolic volume; EF, ejection fraction; ESV, end-systolic volume; LA, left atrium; STD, standard deviation; SV, stroke volume.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 4
Left Atrial Function, Volume and Diameter (Absolute and Indexed Values) in Normal Patients and Patients with Atrial Fibrillation (Mean ± SD, 95% Confidence Interval)
Groups Normal Paroxysmal AF Nonparoxysmal AF_P_ Value ∗ Females Absolute values N 37 35 10 LA EDV (mL) 74 ± 18 (68–80) 104 ± 29 (94–114) 115 ± 33 (95–135) <.0001 † LA ESV (mL) 34 ± 11 (30–37) 64 ± 26 (55–73) 105 ± 30 (86–124) <.0001 † LA SV (mL) 40 ± 10 (37–43) 40 ± 14 (35–45) 11 ± 6 (7–15) <.0001 † LA EF (%) 55 ± 7 (53–57) 39 ± 14 (34–44) 9 ± 5 (6–12) <.0001 † LA diameter (mm) 31 ± 4 (30–32) 38 ± 6 (36–40) 45 ± 5 (42–48) <.0001 † Indexed to BSA LA EDV/BSA (mL/m 2 ) 40 ± 9 (37–43) 56 ± 16 (51–61) 57 ± 20 (45-69) <.0001 † LA ESV/BSA (mL/m 2 ) 18 ± 6 (16–20) 35 ± 14 (30–40) 52 ± 18 (41–63) <.0001 † LA SV/BSA (mL/m 2 ) 22 ± 5 (20–24) 21 ± 7 (19–23) 5 ± 3 (3–7) <.0001 † LA diameter/BSA (mm/m 2 ) 16 ± 2 (15–17) 20 ± 4 (19–21) 22 ± 3 (20–24) <.0001 † Males Absolute values N 39 78 33 LA EDV (mL) 86 ± 20 (80–92) 110 ± 30 (103–117) 137 ± 36 (125–149) <.0001 † LA ESV (mL) 46 ± 13 (42–50) 67 ± 25 (61–72) 115 ± 38 (102–128) <.0001 † LA SV (mL) 39 ± 11 (35–42) 42 ± 14 (39–45) 20 ± 16 (15–25) <.0001 † LA EF (%) 46 ± 7 (44–48) 40 ± 12 (37–43) 20 ± 14 (15–25) <.0001 † LA diameter (mm) 31 ± 4 (30–32) 39 ± 7 (37–41) 47 ± 6 (45–49) <.0001 † Indexed to BSA LA EDV/BSA (mL/m 2 ) 41 ± 9 (38–44) 50 ± 14 (47–53) 60 ± 17 (54–66) <.0001 † LA ESV/BSA (mL/m 2 ) 22 ± 6 (20–24) 30 ± 11 (28–32) 50 ± 18 (44–56) <.0001 † LA SV/BSA (mL/m 2 ) 19 ± 5 (17–21) 19 ± 6 (18–20) 8 ± 7 (6–10) <.0001 † LA diameter/BSA (mm/m 2 ) 14 ± 2 (13–15) 18 ± 3 (17–19) 20 ± 3 (19–21) <.0001 †
AF, atrial fibrillation; BSA, body surface area; EDV, end-diastolic volume; ESV, end-systolic volume; LA, left atrium; SD, standard deviation; SV, stroke volume.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
AF and LA Ejection Fraction
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Predictors of LA Volume
Get Radiology Tree app to read full this article<
LA Measurements and Presence of AF
Get Radiology Tree app to read full this article<
Table 5
Unadjusted and Adjusted ORs for LA MDCT Variables Used as Associations with the Presence of AF (AF vs. Normal Patients)
LA MDCT Unadjusted OR (95% CI) ∗ P Value Adjusted OR (95% CI) ∗ P Value Absolute LA MDCT values Maximum volume 1.05 (1.03–1.06) <.0001 † 1.03 (1.01–1.05) .0005 † Minimum volume 1.08 (1.05–1.05) <.0001 † 1.06 (1.03–1.08) .0001 † Stroke volume 0.98 (0.96–0.99) .02 † 0.99 (0.96–1.02) .49 Ejection fraction 0.91 (0.88–0.93) <.0001 † 0.93 (0.89–0.97) .0005 † Diameter 1.32 (1.23–1.42) <.0001 † 1.29 (1.17–1.42) <.0001 † Indexed LA MDCT values Maximum volume 1.08 (1.05–1.11) <.0001 † 1.06 (1.03–1.10) .0003 † Minimum volume 1.16 (1.11–1.21) <.0001 † 1.12 (1.06–1.09) <.0001 † Stroke volume 0.93 (0.89–0.97) .0004 † 0.97 (0.92–1.03) .31 Diameter 3.62 (0.76–17.21) .11 3.37 (0.55–20.82) .19
AF, atrial fibrillation; CI, confidence interval; LA, left atrium; MDCT, multidetector computed tomography; OR, odds ratio.
Adjusted absolute values for hypertension, coronary artery disease, age, sex, body surface area and body mass index. Adjusted indexed values for coronary artery disease, hypertension, gender and age.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
MDCT LA Measurements and AF Chronicity
Get Radiology Tree app to read full this article<
Table 6
Unadjusted and Adjusted ORs for LA MDCT Variables Used as Associations with AF Chronicity (Nonparoxysmal vs. Paroxysmal AF)
LA MDCT Unadjusted OR (95% CI) ∗ P Value Adjusted OR (95% CI) ∗ P Value Absolute LA MDCT values Maximum volume 1.31 (1.03–1.65) .02 † 1.48 (1.12–1.95) .005 † Minimum volume 0.79 (0.63–0.99) .04 † 0.71 (0.54–0.93) .01 † Stroke volume 0.65 (0.5–0.85) .002 † 0.55 (0.39–0.75) .0009 † Ejection fraction 1.08 (0.97–1.22) .35 1.12 (0.93–1.33) .21 Diameter 1.12 (1.04–1.25) .04 † 1.15 (0.98–1.35) .07 Indexed LA MDCT values Maximum volume 1.66 (1.06–2.61) .01 † 2.42 (1.43–4.08) .0009 † Minimum volume 0.61 (0.39–0.94) .03 † 0.43 (0.26–0.73) .001 † Stroke volume 0.46 (0.29–0.73) .001 † 0.31 (0.17–0.55) <.0001 † Diameter 1.03 (0.83–1.27) .89 1.22 (0.93–1.59) .15
AF, atrial fibrillation; CI, confidence interval; LA, left atrium; MDCT, multidetector computed tomography; OR, odds ratio.
Adjusted absolute values for hypertension, coronary artery disease, age, sex, body surface area and body mass index. Adjusted indexed values for coronary artery disease, hypertension, gender and age.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Traditional Risk Factors and Nonparoxysmal AF
Get Radiology Tree app to read full this article<
Discussion
Main Findings
Get Radiology Tree app to read full this article<
MDCT LA Measures and Presence of AF
Get Radiology Tree app to read full this article<
MDCT LA Measures and Chronicity of AF
Get Radiology Tree app to read full this article<
LA Diameter Versus LA Maximum Volume
Get Radiology Tree app to read full this article<
MDCT Measures and Traditional Risk Factors
Get Radiology Tree app to read full this article<
Strengths and Limitations
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Clinical Implications
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Go A.S., Hylek E.M., Phillips K.A., et. al.: Prevalence of diagnosed atrial fibrillation in adults: national implications for rhythm management and stroke prevention: the AnTicoagulation and Risk Factors in Atrial Fibrillation (ATRIA) Study. JAMA 2001; 285: pp. 2370-2375.
2. Heeringa J., van der Kuip D., Hofman A., et. al.: Prevalence, incidence and lifetime risk of strial fibrillation: the Rotterdam study. Eur Heart J 2006; 27: pp. 949-953.
3. European Heart Rhythm Association, Heart Rhythm Society, Fuster V., Rydén L.E., Cannom D.S., et. al., American College of Cardiology, American Heart Association Task Force on Practice Guidelines, European Society of Cardiology Committee for Practice Guidelines, Writing Committee to Revise the 2001 Guidelines for the Management of Patients With Atrial Fibrillation: ACC/AHA/ESC 2006 guidelines for the management of patients with atrial fibrillation—executive summary: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and the European Society of Cardiology Committee for Practice Guidelines (Writing Committee to Revise the 2001 Guidelines for the Management of Patients With Atrial Fibrillation). J Am Coll Cardiol 2006; 48: pp. 854-906.
4. European Heart Rhythm Association (EHRA), European Cardiac Arrhythmia Society (ECAS), American College of Cardiology (ACC), American Heart Association (AHA), Society of Thoracic Surgeons (STS), Calkins H., Brugada J., Packer D.L., et. al.: HRS/EHRA/ECAS expert consensus statement on catheter and surgical ablation of atrial fibrillation: recommendations for personnel, policy, procedures and follow-up. A report of the Heart Rhythm Society (HRS) Task Force on catheter and surgical ablation of atrial fibrillation. Heart Rhythm 2007; 4: pp. 816-861.
5. Haïssaguerre M., Jais P., Shah D.C., et. al.: Spontaneous initiation of atrial fibrillation by ectopic beats originating in the pulmonary veins. N Engl J Med 1998; 339: pp. 659-666.
6. Tan A.Y., Chen P.S., Chen L.S., et. al.: Autonomic nerves in pulmonary veins. Heart Rhythm 2007; 4: pp. S57-S60.
7. Lemola K., Desjardins B., Sneider M., et. al.: Effect of left atrial circumferential ablation for atrial fibrillation on left atrial transport function. Heart Rhythm 2005; 2: pp. 923-928.
8. Thomas L., Thomas S.P., Hoy M., et. al.: Comparison of left atrial volume and function after linear ablation and after cardioversion for chronic atrial fibrillation. Am J Cardiol 2004; 93: pp. 165-170.
9. Marsan N.A., Tops L.F., Holman E.R., et. al.: Comparison of left atrial volumes and function by real-time three-dimensional echocardiography in patients having catheter ablation for atrial fibrillation with persistence of sinus rhythm versus recurrent atrial fibrillation three months later. Am J Cardiol 2008; 102: pp. 847-853.
10. Jeevanantham V., Ntim W., Navaneethan S.D., et. al.: Meta-analysis of the effect of radiofrequency catheter ablation on left atrial size, volumes and function in patients with atrial fibrillation. Am J Cardiol 2010; 105: pp. 1317-1326.
11. Lo L.W., Lin Y.J., Tsao H.M., et. al.: The impact of left atrial size on long-term outcome of catheter ablation of chronic atrial fibrillation. J Cardiovasc Electrophysiol 2009; 20: pp. 1211-1216.
12. Tsang M.Y.C., Barnes M.E., Tsang T.S.M.: Left atrial volume: clinical value revisited. Curr Cardiol Rep 2012; 14: pp. 374-380.
13. Manning W.J., Silwerman D.I., Katz S.E., et. al.: Atrial ejection force: a noninvasive assessment of atrial systolic function. J Am Coll Cardiol 1993; 22: pp. 221-225.
14. Marchese P., Malavasi V., Rossi L., et. al.: Indexed left atrial volume is superior to left atrial diameter in predicting nonvalvular atrial fibrillation recurrence after successful cardioversion: a prospective study. Echocardiography 2012; 29: pp. 276-284.
15. Tsang T.S., Gersh B.J., Appleton C.P., et. al.: Left ventricular diastolic dysfunction as a predictor of first diagnosed nonvalvular atrial fibrillation in 840 elderly men and women. J Am Coll Cardiol 2002; 40: pp. 1636-1644.
16. Nagarakanti R., Ezekowitz M.: Diastolic dysfunction and atrial fibrillation. J Interv Card Electrophysiol 2008; 22: pp. 111-118.
17. Wilson P.W., D’Agostino R.B., Levy D., et. al.: Prediction of coronary heart disease using risk factor categories. Circulation 1998; 97: pp. 1837-1847.
18. Stojanovska J., Cronin P., Patel S., et. al.: Reference normal absolute and indexed values from ECG-gated MDCT:left atrial volume, function, and diameter. Am J Roentgenol 2011; 197: pp. 631-637.
19. WHO. Physical status: the use and interpretation of anthropometry. Report of WHO Expert Consultation. WHO Technical Report Series Number 854. Geneva: World Health Organization, 1995.
20. Mosteler R.D.: Simplified calculation of body surface area. N Engl J Med 1987; 317: pp. 1098.
21. Egan B.M., Zhao Y., Axon R.N.: US trends in prevalence, awareness, treatment, and control of hypertension, 1988-2008. JAMA 2010; 303: pp. 2043-2050.
22. Mahabadi A.A., Massaro J.M., Rosito G.A., et. al.: Association of pericardial fat, intrathoracic fat and visceral abdominal fat with cardiovascular disease burden: the Framingham Heart Study. Eur Heart J 2009; 30: pp. 850-856.
23. Petersen P., Kastrup J., Brinch K., et. al.: Relation between left atrial dimension and duration of atrial fibrillation. Am J Cardiol 1987; 60: pp. 382-384.
24. Kuppahally S.S., Akoum N., Burgon N.S., et. al.: Left atrial strain and strain rate in patients with paroxysmal and persistent atrial fibrillation: relationship to left atrial structural remodeling detected by delayed-enhancement MRI. Circ Cardiovasc Imaging 2010; 3: pp. 231-239.
25. Yoon J.H., Moon J., Chung H.M., et. al.: Left atrial function assessed by Doppler echocardiography rather then left atrial volume predicts recurrence in patients with paroxysmal atrial fibrillation. Clin Cardiol 2013; 36: pp. 235-240.
26. Marchese P., Bursi F., Delle Donne G., et. al.: Indexed left atrial volume predicts the recurrence of non-valvular atrial fibrillation after successful cardioversion. Eur J Echocardiogr 2011; 12: pp. 214-221.
27. Hof I., Chilukuri K., Arbab-Zadeh A., et. al.: Does left atrial volume and pulmonary venous anatomy predict the outcome of catheter ablation of atrial fibrillation?. J Cardiovasc Electrophysiol 2009; 20: pp. 1005-1010.
28. Abecasis J., Dourado R., Ferreira A., et. al.: Left atrial volume calculated by multi-detector computed tomography may predict successful pulmonary vein isolation in catheter ablation of atrial fibrillation. Europace 2009; 11: pp. 1289-1294.
29. Tsang T.S., Barnes M.E., Bailey K.R., et. al.: Left atrial volume: important risk marker of incident atrial fibrillation in 1655 older men and women. Mayo Clin Proc 2001; 76: pp. 467-475.
30. Leung D.Y., Chi C., Allman C., et. al.: Prognostic implications of left atrial volume index in patients in synus rhythm. Am J Cardiol 2010; 105: pp. 1635-1639.
31. Abhayaratna W.P., Seward J.B., Appleton C.P., et. al.: Left atrial size: physiologic determinants and clinical applications. J Am Coll Cardiol 2006; 47: pp. 2357-2363.
32. Chekakie M.O., Welles C.C., Metoyer R., et. al.: Pericardial fat is independently associated with human atrial fibrillation. JACC 2010; 56: pp. 784-788.