
Rationale and Objectives
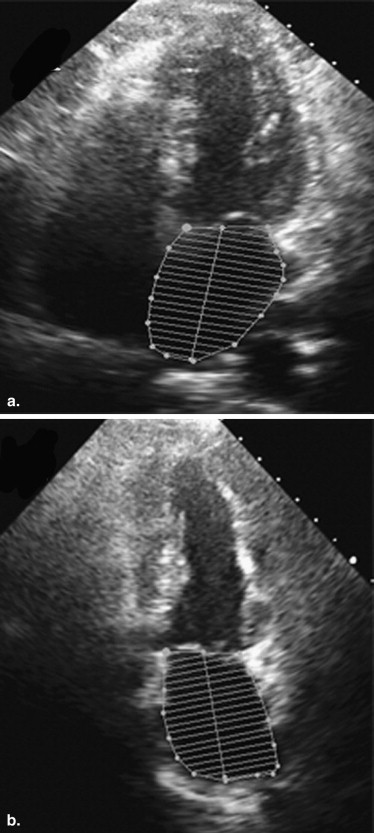
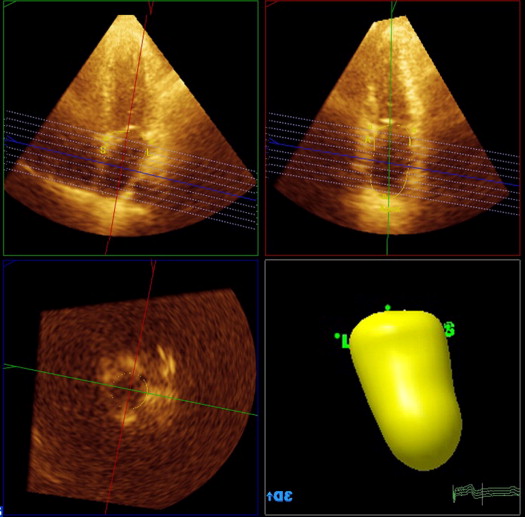
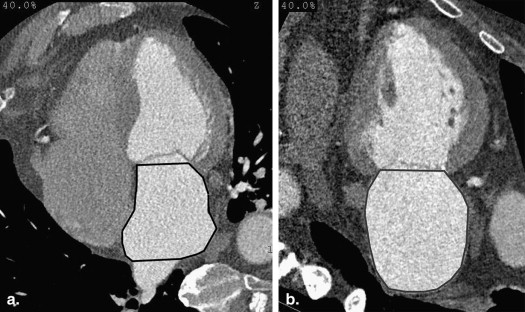
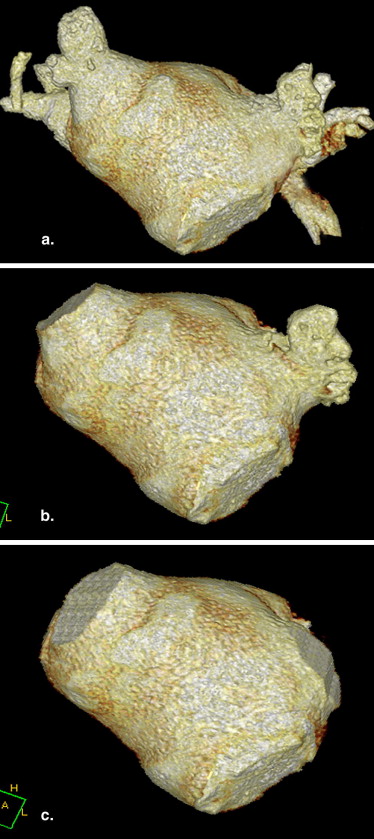
Left atrial volume (LAV) measurement by conventional two-dimensional (2D) transthoracic echocardiography (TTE) may be limited by the geometric model, by suboptimal definition of left atrial endocardium, or by chamber foreshortening. Three-dimensional (3D) TTE is posited to eliminate chamber foreshortening, and LAV measurement by 3D TTE should be more reflective of true LAV. The aim of this study was to compare conventional 2D TTE and newer 3D TTE for measurements of LAV to multidetector computed tomographic (MDCT) measurements using automated chamber reconstruction (ACR).
Materials and Methods
Twenty-two subjects consented to undergo 2D TTE and 3D TTE immediately prior to or following coronary computed tomographic angiography. LAV was calculated from 2D TTE using the area-length method (ALM) and from 3D TTE with the ALM as well as with a 3D model. Electrocardiographically gated coronary computed tomographic angiography was performed in helical mode. LAV was measured using the ALM as well as ACR.
Results
LAV was significantly smaller by 2D TTE (80 ± 21 mL) and 3D-TTE (90 ± 24 mL with the ALM, 61 ± 16 mL with the 3D model) compared to MDCT ACR (120 ± 30 mL) ( P < .01). Correlation between MDCT ALM and MDCT ACR was excellent (mean Δ = −1.4 ± 14 mL, r = 0.91). Correlation with MDCT ACR was no better for 3D TTE ( r = 0.80) than for 2D TTE ( r = 0.80).
Conclusions
LAV is underestimated by both 2D TTE and 3D TTE relative to coronary computed tomographic angiography. Excellent agreement between the ALM and ACR with MDCT imaging suggests that the geometric model plays a negligible role in the underestimation of LAV. Underestimation of LAV by echocardiography is likely related to suboptimal definition of left atrial contour.
Left atrial size is an important marker for a variety of clinical disease states. Elevated left atrial size predicts diastolic dysfunction , the severity of mitral regurgitation , and the likelihood of success of pulmonary vein isolation in treating atrial fibrillation . Increased left atrial size portends poorer outcomes in patients with atrial fibrillation , myocardial infarction , and dilated cardiomyopathy . Thus, accurate measurement of left atrial size is of primary importance.
Historically, computed tomographic (CT) imaging and magnetic resonance imaging (MRI) have served as gold standards for left atrial volume (LAV), and two-dimensional (2D) transthoracic echocardiography (TTE) was validated against these reference standards . Echocardiography is currently the most common modality used to measure the left atrium because of its lower cost, portability, and universal availability. The current recommended standard to estimate LAV as defined by the American Society of Echocardiography uses an ellipsoid geometric model derived from two orthogonal apical views with the biplane area-length method (ALM) . Unfortunately, because the ALM depends on the acquisition of two nonforeshortened images, and on a geometric estimate, it is prone to errors.
Get Radiology Tree app to read full this article<
Methods
Patient Selection
Get Radiology Tree app to read full this article<
Echocardiography
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Cardiac MDCT Imaging
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Table 1
Baseline Characteristics
Variable Value Number of subjects 22 Age (y), mean ± standard deviation 51 ± 13 Men 59% Indication for MDCT imaging Abnormal stress test results 18 Interrupted aortic arch 1 Ventricular septal defect 1 Atrial septal defect 1 Right ventricular mass 1
MDCT, multidetector computed tomographic.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 2
Comparison of Different 2DE and 3DE Methods of Measuring the Left Atrium to the Reference Standard of MDCT ACR
Method Mean ± Standard Deviation (mL) Correlation ( r ) Mean Difference (mL) Limits of Agreement (mL) MDCT ACR (reference standard) 120 ± 30 MDCT ALM 115 ± 31 0.91 −1.4 26 to −29 2DE ALM 80 ± 21 0.80 −38 2 to −78 3DE SAV 61 ± 16 0.80 −58 −19 to −98 3DE ALM 90 ± 24 0.80 −28 16 to −71
ACR, automated chamber reconstruction; ALM, area-length method; MDCT, multidetector computed tomographic; SAV, semiautomated volume; 3DE, three-dimensional echocardiographic; 2DE, two-dimensional echocardiographic.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 3
Interobserver Variability
Method Interobserver Variability 2DE ALM 11% 3DE SAV 9% MDCT ALM 9% MDCT ACR 4%
ACR, automated chamber reconstruction; ALM, area-length method; MDCT, multidetector computed tomographic; SAV, semiautomated volume; 3DE, three-dimensional echocardiographic; 2DE, two-dimensional echocardiographic.
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Limitations
Get Radiology Tree app to read full this article<
Conclusions
Get Radiology Tree app to read full this article<
References
1. Nagueh S.F., Appleton C.P., Gillebert T.C., et. al.: Recommendations for the evaluation of left ventricular diastolic function by echocardiography. J Am Soc Echocardiogr 2009; 22: pp. 107-133.
2. Zoghbi W.A., Enriquez-Sarano M., Foster E., et. al.: American Society of Echocardiography. Recommendations for evaluation of the severity of native valvular regurgitation with two-dimensional and Doppler echocardiography. J Am Soc Echocardiogr 2003; 16: pp. 777-802.
3. Montefusco A., Biasco L., Blandino A., et. al.: Left atrial volume at MRI is the main determinant of outcome after pulmonary vein isolation plus linear lesion ablation for paroxysmal-persistent atrial fibrillation. J Cardiovasc Med (Hagerstown) 2010; 11: pp. 593-598.
4. Benjamin E.J., D’Agostino R.B., Belanger A.J., et. al.: Left atrial size and the risk of stroke and death: the Framingham heart study. Circulation 1995; 92: pp. 835-841.
5. Bolca O., Akdemir O., Eren M., et. al.: Left atrial maximum volume is a recurrence predictor in lone atrial fibrillation: an acoustic quantification study. Jpn Heart J 2002; 43: pp. 241-248.
6. Di Tullio M.R., Sacco R.L., Sciacca R.R., et. al.: Left atrial size and the risk of ischemic stroke in an ethnically mixed population. Stroke 1999; 30: pp. 2019-2024.
7. Moller J.E., Hillis G.S., Oh J.K., et. al.: Left atrial volume: a powerful predictor of survival after acute myocardial infarction. Circulation 2003; 107: pp. 2207-2212.
8. Beinart R., Boyko V., Schwammenthal E., et. al.: Long-term prognostic significance of left atrial volume in acute myocardial infarction. J Am Coll Cardiol 2004; 44: pp. 327-334.
9. Modena M.G., Muia N., Sgura F.A., et. al.: Left atrial size is the major predictor of cardiac death and overall clinical outcome in patients with dilated cardiomyopathy: a long-term follow-up study. Clin Cardiol 1997; 20: pp. 553-560.
10. Kircher B., Abbott J.A., Pau S., et. al.: Left atrial volume determination by biplane two-dimensional echocardiography: validation by cine computed tomography. Am Heart J 1991; 121: pp. 864-871.
11. Jarvinen V., Kupari M., Hekali P., et. al.: Assessment of left atrial volumes and phasic function using cine magnetic resonance imaging in normal subjects. Am J Cardiol 1994; 73: pp. 1135-1138.
12. Lang R.M., Bierig M., Devereux R.B., et. al.: Chamber Quantification Writing Group; American Society of Echocardiography’s Guidelines and Standards Committee; European Association of Echocardiography. Recommendations for chamber quantification: a report from the American Society of Echocardiography’s Guidelines and Standards Committee and the Chamber Quantification Writing Group, developed in conjunction with the European Association of Echocardiography, a branch of the European Society of Cardiology. J Am Soc Echocardiogr 2005; 18: pp. 1440-1463.
13. Rodevand O., Bjornerheim R., Ljosland M., et. al.: Left atrial volumes assessed by three and two-dimensional echocardiography compared to MRI estimates. Int J Card Imaging 1999; 15: pp. 397-410.
14. Keller A.M., Gopal A.S., King D.L.: Left and right atrial volume by freehand three-dimensional echocardiography: in vivo validation using magnetic resonance imaging. Eur J Echocardiogr 2000; 1: pp. 55-65.
15. Artang R., Migrino R.Q., Harmann L., et. al.: Left atrial volume measurement with automated border detection by 3-dimensional echocardiography: comparison with magnetic resonance imaging. Cardiovasc Ultrasound 2009; 7: pp. 16.
16. Koka A.R., Yau J., Van Why C., et. al.: Underestimation of left atrial size measured with transthoracic echocardiography compared with 3D MDCT. AJR Am J Roentgenol 2010; 194: pp. W375-W381.
17. Christiaens L., Lequeux B., Ardilouze P., et. al.: A new method for measurement of left atrial volumes using 64-slice spiral computed tomography: comparison with two-dimensional echocardiographic techniques. Int J Cardiol 2009; 131: pp. 217-224.