
Rationale and Objectives
Competency in ultrasound (US) imaging and US-guided procedures is often difficult for medical students and residents to master. The use of simulation training has been strongly encouraged but the quality of phantom models available for US-guided procedures is limited. As a feasible alternative, we describe the innovative use of a lightly embalmed cadaver for realistic practice of common interventional radiology (IR) procedures prior to direct patient care.
Materials and Methods
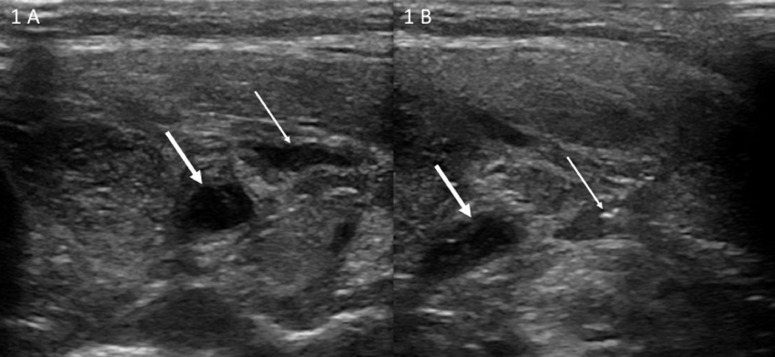
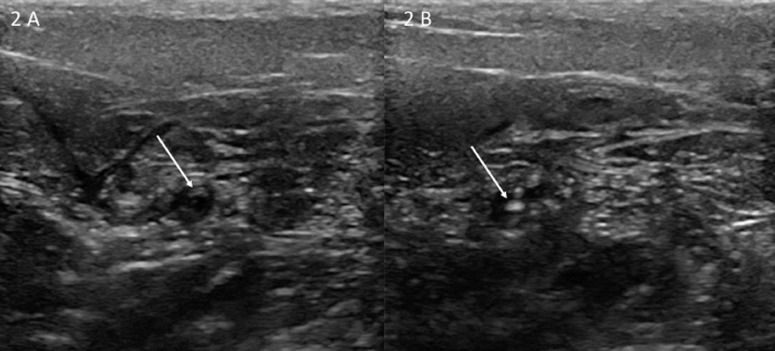
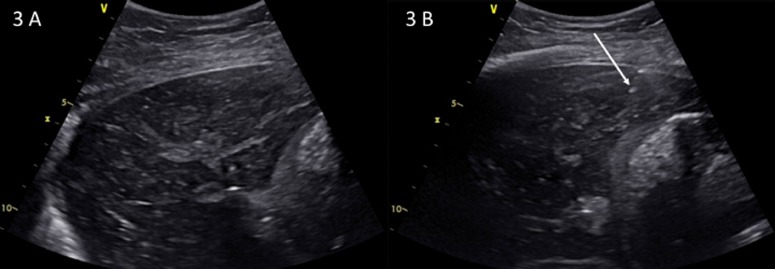
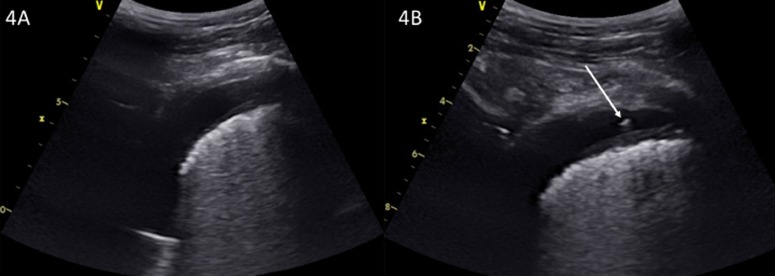
Lightly embalmed cadavers were positioned as patients would be in the IR suite: supine, prone, and erect seated position. Lidocaine was injected and visualized under standard percutaneous techniques and sonographic guidance was used to simulate common US-guided procedures performed in IR including liver biopsy, kidney biopsy, thoracentesis, and vascular access.
Results
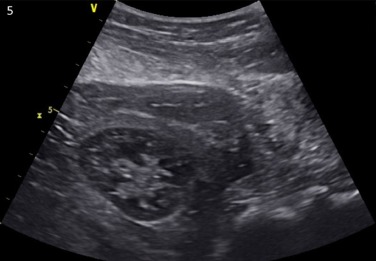
The ability to position cadavers was a key factor that allowed entire procedures to be simulated. Medical students with very limited exposure to US imaging and diagnostic radiology residents with minimal exposure to US imaging successfully completed common US-guided procedures. Arterial and venous vascular access was obtained. Wires were passed and catheters easily placed via both access sites. The texture of the tissue layers provided realistic feedback for the trainees as they advanced the needle or dilated the tissues. Images from each simulated procedure resembled images expected in a living patient.
Conclusion
Lightly embalmed cadavers are an innovative and feasible tool to simulate common IR US-guided procedures in a realistic fashion for deliberate practice in advance of first-attempt encounters with patients.
Introduction
Competency in ultrasound (US) imaging and US-guided procedures is a fundamental skill required for interventional radiology (IR) physicians but often difficult for trainees to master. Although the use of US-guided procedures in the field of medicine has drastically increased in recent years, students are minimally exposed to US during medical school ( ). IR procedures are classically taught via literature, simulations, and demonstration before trainees attempt procedures under direct observation. Attempting IR procedures when patients are awake or minimally sedated creates apprehension in patients which in turn increases the resident’s anxiety and can lead to mistakes in technique, medical errors, and less effective teaching. As a learning experience, this approach limits open communication, instruction, and experimentation the resident needs to develop the appropriate skill set.
The use of simulation to achieve excellence and safety in IR patient care has been strongly encouraged ( ). Hours spent in deliberate practice, intentionally repeating an activity in order to improve performance or master a task, have correlated with the development of expertise. Simulation allows deliberate practice in a safe environment, as often as needed for mastery learning, without jeopardizing patient safety ( ). Combined with immediate feedback and self-evaluation, deliberate practice requires effort, and, though not innately enjoyable, can reduce training time and be more effective than nonfocused training ( ). With permission to fail and correct mistakes remote from patients, novice operators can practice common percutaneous procedures that range in complexity from superficial skin punctures to biopsies, aspirations, and central venous access. Likewise, experts can refresh old skills and learn new ones.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Materials and Methods
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 1
First-Year Medical Student (M1) Evaluation of US-Guided Central Venous Line Placement on Lightly Embalmed Cadavers (2014)
Mean ± Standard error of the mean ( n = 16) 1. The session was well organized and material presented in a logical sequence 4.47 ± 0.14 2. The lightly embalmed cadaver was a great learning tool 5.00 ± 0.00 3. The information presented was clinically relevant 4.89 ± 0.07 4 The presenter was knowledgeable in the topic 4.84 ± 0.09 5. The overall quality of this session was outstanding 4.58 ± 0.14 6. I would recommend this session to M1 students next year 4.79 ± 0.12
Rating scale: 5—Strongly agree; 4—Agree; 3—Neither Agree or Disagree; 2—Disagree; 1—Strongly Disagree.
Table 2
First-Year Medical Student (M1) Evaluation of US Guided Liver and Kidney Biopsy on Lightly Embalmed Cadavers (2018)
Mean ± Standard error of the mean ( n = 29) 1. The session was well organized and material presented in a logical sequence 4.76 ± 0.44 2. The lightly embalmed cadaver was a great learning tool 4.93 ± 0.26 3. The information presented was clinically relevant 4.86 ± 0.44 4. The presenter was knowledgeable in the topic 4.90 ± 0.31 5. The overall quality of this session was outstanding 4.76 ± 0.44 6. I would recommend this session to M1 students next year 4.90 ± 0.31 7. As a result of this session, I feel more confident in my ability to perform US-guided procedures. 4.59 ± 0.57
Rating scale: 5 —Strongly agree; 4—Agree; 3—Neither Agree or Disagree; 2—Disagree; 1—Strongly Disagree.
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Appendix A
Medical Student Comments and Suggestions
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Miller R, Ho H, Ng V, et. al.: Introducing a fresh cadaver model for ultrasound-guided central venous access training in undergraduate medical education. West J Emerg Med 2016; 17: pp. 362-366.
2. Hoffman L, Wadman MC, Erickson T, et. al.: Self-reported EM residency applicant attitudes towards a procedural cadaver laboratory curriculum. West J Emerg Med 2008; 9: pp. 141-145.
3. Gould D: Using simulation for interventional radiology training. Br J Radiol 2010; 83: pp. 546-553.
4. Ericsson KA.: Deliberate practice and acquisition of expert performance: a general overview. Acad Emerg Med 2008; 15: pp. 988-994.
5. Kneebone R.: Evaluating clinical simulations for learning procedural skills: a theory-based approach. Acad Med 2005; 23: pp. 549-553.
6. Levine RL, Kives S, Cathey G, et. al.: The use of lightly embalmed (fresh tissue) cadavers for resideny laproscopic training. J Minim Invasive Gynecol 2006; 13: pp. 451-456.
7. Fulton N, Buethe J, Gollamudi J, et. al.: Simulation-based training may improve resident skill in ultrasound-guided biopsy. AJR 2016; 207: pp. 1329-1333.
8. Passiment M, Sacks H, Huang G: Medical simulation in medical education: results of an AAMC survey. Assoc Am Med Coll Rep 2011; Available at: https://www.aamc.org/download/259760/data Accessed February 7, 2017
9. Baadh A, Fadl A, Georgiou N, et. al.: A pilot program for use of a homemade phantom for CT biopsy simulation training. JVIR 2015; 26: pp. S167.
10. Ball R, Scouras N, Orebaugh S, et. al.: Randomized, prospective, observational simulation study comparing residents’ needle-guided vs free-hand ultrasound technique for central venous catheter access. Br J Anaesth 2012; 108: pp. 72-79.
11. Cook DA, Hatala R, Brydges R, et. al.: Technology-enhanced simulation for health professions education: a systematic review and meta-analysis. JAMA 2011; 306: pp. 978-988.
12. Lewandowski W, Gould D. A summary of the subjective opinions of interventional radiologist regarding selected medical simulations. Available from: http://www.whichinterventionaldevice.com/product-categories/simulators.aspx . Accessed February 13, 2017.
13. Anderson SD: Practical light embalming technique for use in the surgical fresh tissue dissection laboratory. Clin Anat 2006; 19: pp. 8-11.
14. Cork K: UNMC’s ‘lightly embalmed’ cadaver program provides innovative learning tool. UNMC Depart Pharmacol/Exp\ Neurosci 2015; Available at https://www.unmc.edu/news.cfm?match=16295 Accessed April 12, 2018
15. Wadman MC, Lomneth CS, Hoffman LH, et. al.: Assessment of a new model for femoral ultrasound-guided central venous access procedural training: a pilot study. Acad Emerg Med 2010; 17: pp. 88-92.
16. Wadman M, Nicholas TA, Bernhagen MA, et. al.: A comparison of an integrated suction blade versus a traditional videolaryngoscope blade in the endotracheal intubation of a hemorrhagic cadaver model: a pilot study. Stud Health Technol Inform 2012; 173: pp. 534-536.
17. Keim Janssen SA, VanderMeulen SP, Shostrom VK, et. al.: Enhancement of anatomical learning and developing clinical competence of first-year medical and allied health profession students. Anat Sci Educ 2014; 7: pp. 181-190.
18. Adhikari S, Zeger W, Wadman M, et. al.: Assessment of a human cadaver model for training emergency medicine residents in the ultrasound diagnosis of pneumothorax. Biomed Res Int 2014;
19. Siragusa DA, Cardella JF, Hieb RA, et. al.: Requirements for training in interventional radiology. JVIR 2013; 24: pp. 1609-1612.