
Rationale and Objectives
3-Bromopyruvate (3-BrPA), an hexokinase II inhibitor, is known to have high necrotic rate in hyperglycolytic liver tumor models without apparent damage to the normal liver parenchyma. The toxicity of intra-arterial delivery of 3-BrPA in various concentrations has not been specifically investigated using a normal rabbit model.
Materials and Methods
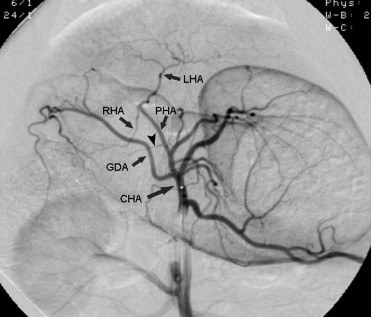
Twenty rabbits treated with intra-arterial 3-BrPA were divided into four groups according to its dose and infusion level: 1 mM at the left hepatic artery (group I), 5 mM at the left hepatic artery (group II), 25 mM at the left hepatic artery (group III), and 25 mM at the common hepatic artery (group IV). After selective catheterization, 30 ml of 3-BrPA was infused for 2 minutes. As a control group, five rabbits were treated with normal saline. During 1-week follow-up, toxicities were evaluated with blood laboratory results, mortality, and histopathologic examination.
Results
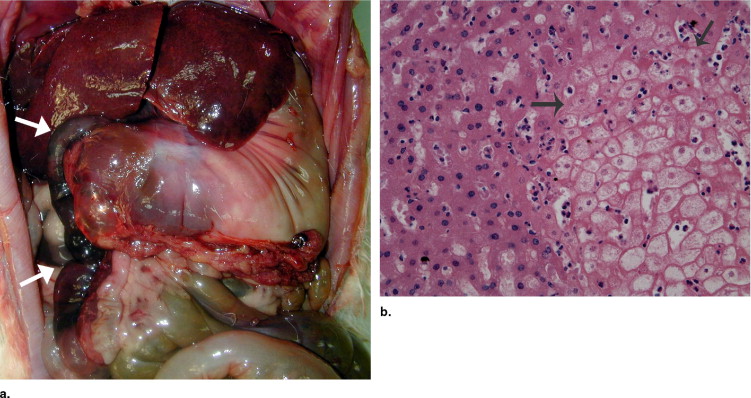
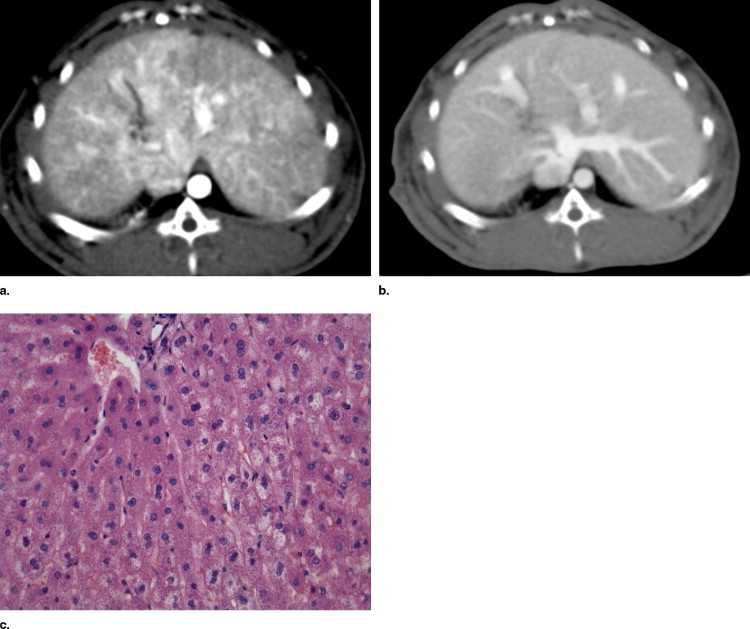
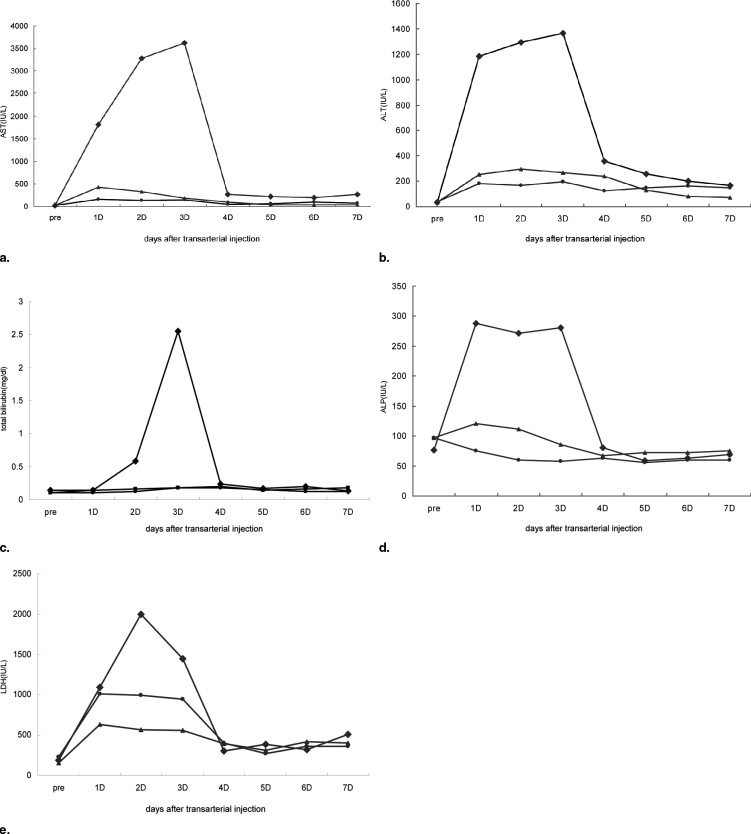
All 10 rabbits treated with 25 mM 3-BrPA and 2 rabbits treated with 5 mM 3-BrPA died within 3 days after treatment. In 10 of the 12 deaths, hemorrhagic pyloric or duodenal necrosis was noted. Hepatotoxicities on blood laboratory results were dose dependent but transient in the surviving rabbits.
Conclusion
Selective intra-arterial administration of 25 mM 3-BrPA can cause considerable toxicities not only in the liver but also in the gastrointestinal system and are dose dependent and can cause death in high doses.
Hepatocellular carcinoma (HCC) is the fifth most common cancer, and the third most common cause of cancer-related death in the world ( ). Because of the advanced stage of the disease and associated liver cirrhosis at its initial presentation, only a minority of patients are eligible for curative treatments such as surgical excision or local ablation therapies such as radiofrequency ablation and percutaneous ethanol injection ( ). Therefore, transcatheter arterial approach has been widely investigated as a palliative treatment for HCC, which includes hepatic arterial infusion chemotherapy and transcatheter arterial chemoembolization (TACE) ( ). Recently, survival benefit of TACE has been proved by prospective randomized clinical trial ( ). However, the therapeutic efficacy of TACE is still limited and deterioration of liver function is unavoidably associated.
As a new concept for anticancer therapy, blocking of cancer energy metabolism by selective hexokinase II inhibition has been proposed ( ). Hexokinase is the first-step enzyme of glucose metabolism. Among hexokinase isotypes, hexokinase II is overexpressed in tumor cells to produce ATP and cell building blocks for uncontrolled tumor overgrowth. Theoretically, selective inhibition of hexokinase II may lead to tumor necrosis without normal tissue damage ( ).
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Materials and methods
Experimental Animal and Study Design
Get Radiology Tree app to read full this article<
Preparation of 3-BrPA Solution
Get Radiology Tree app to read full this article<
Procedures for Intra-arterial Administration of 3-BrPA and Normal Saline
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Evaluation of Hepatotoxicity
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Conclusion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Montalto G., Cervello M., Giannitrapani L., et. al.: Epidemiology, risk factors, and natural history of hepatocellular carcinoma. Ann N Y Acad Sci 2002; 963: pp. 13-20.
2. Parkin D.M., Bray F., Ferlay J., et. al.: Estimating the world cancer burden: GLOBOCAN 2000. Int J Cancer 2001; 94: pp. 153-156.
3. Venook A.P.: Treatment of hepatocellular carcinoma: Too many options?. J Clin Oncol 1994; 12: pp. 1323-1334.
4. Ramsey D.E., Kernagis L.Y., Soulen M.C., Geschwind J.F.: Chemoembolization of hepatocellular carcinoma. J Vasc Interv Radiol 2002; 13: pp. S211-S221.
5. Llovet J.M., Real M.I., Montana X., et. al.: Arterial embolisation or chemoembolisation versus symptomatic treatment in patients with unresectable hepatocellular carcinoma: A randomized controlled trial. Lancet 2002; 359: pp. 1734-1739.
6. Ko Y.H., Pedersen P.L., Geschwind J.F.: Glucose catabolism in the rabbit VX2 tumor model for liver cancer: Characterization and targeting hexokinase. Cancer Lett 2001; 173: pp. 83-91.
7. Bustamante E., Morris H.P., Pedersen P.L.: Energy metabolism of tumor cells. J Biol Chem 1981; 256: pp. 8699-8704.
8. Geschwind J.F., Ko Y.H., Torbenson M.S., et. al.: Novel therapy for liver cancer: Direct intra-arterial injection of a potent inhibitor of ATP production. Cancer Res 2002; 62: pp. 3909-3913.
9. Dang C.V., Semenza G.L.: Oncogenic alterations of metabolism. Trends Biochem Sci 1999; 24: pp. 68-72.
10. Zasshi Y.: Identification and characterization of hexokinase isozyme predominantly expressed in malignant tumor cells. Yakugaku Zasshi 2000; 120: pp. 657-666.
11. Lee M.G., Pedersen P.L.: Glucose metabolism in cancer: Importance of transcription factor-DNA interactions within a shirt segment of the proximal region of type II hexokinase promoter. J Biol Chem 2003; 278: pp. 41047-41058.
12. Ko Y.H., McFadden B.A.: Alkylation of isocitrate lyase from Escherichia coli by 3-bromopyruvate. Arch Biochem Biophys 1990; 278: pp. 373-380.
13. Gwak G.Y., Yoon J.H., Kim K.M., et. al.: Hypoxia stimulates proliferation of human hepatoma cells through the induction of hexokinase II expression. J Hepatol 2005; 42: pp. 358-364.
14. Ko Y.H., Smith B.L., Wang Y., et. al.: Advanced cancers: eradication in all cases using 3-bromopyruvate therapy to deplete ATP. Biochem Biophys Res Commun 2004; 324: pp. 269-275.
15. Liu D.M., Salem R., Bui J.T., et. al.: Angiographic considerations in patients undergoing liver-directed therapy. J Vasc Interv Radiol 2005; 16: pp. 911-935.
16. Song S.Y., Chung J.W., Lim H.G., et. al.: Nonhepatic arteries originating from the hepatic arteries: Angiographic analysis in 250 patients. J Vasc Interv Radiol 2006; 17: pp. 461-469.