
Rationale and Objectives
To assess the impact of low-concentration contrast medium on vascular enhancement, image quality, and radiation dose of coronary computed tomography (CT) angiography (CCTA) by using prospectively electrocardiography (ECG)-triggered high-pitch spiral acquisition with low tube voltage in combination with iterative reconstruction.
Materials and Methods
One hundred patients (body mass index ≤ 25 kg/m 2 , heart rate ≤ 65 beats per minute) were prospectively randomized to two groups, with 50 patients each, which were differed by contrast medium. All patients underwent prospectively ECG-triggered high-pitch spiral acquisition CCTA (2 × 128 × 0.6 mm, 300 mAs). Group A patients received iopromide 370 (370 mg I/mL), were scanned using 100 kVp, and reconstructed with filtered back projection. Group B patients received Iodixanol 270 (270 mg I/mL), were scanned using low tube voltage of 80 kVp, and reconstructed with iterative reconstruction techniques (IRT). CT attenuation was measured in coronary artery and other anatomic regions. Image quality score, noise, signal-to-noise ratio (SNR), contrast-to-noise ratio (CNR), and radiation dose were calculated and compared.
Results
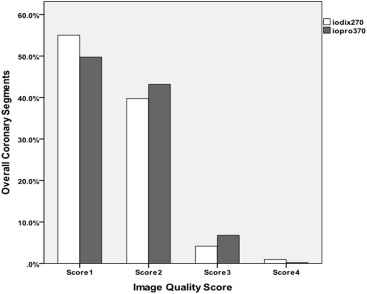
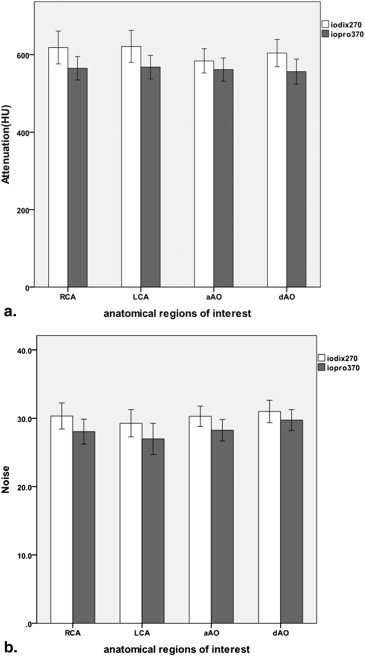
The iodixanol 270 group showed no significant difference in image quality score (1.61 ± 0.69 vs 1.57 ± 0.66; P > .05), CT attenuation ( P > .05), noise ( P > .05), SNR (47.89 ± 14.03 vs 44.37 ± 12.79; P > .05), and CNR (42.38 ± 12.67 vs 38.13 ± 11.38; P > .05) in comparison to the iopromide 370 group but at a significantly lower radiation dose (0.26 ± 0.05 vs 0.57 ± 0.10; P < .001), which reflects dose saving of 54.4%.
Conclusions
Combining IRT with high-pitch spiral acquisition mode and low-tube-voltage technique, a low-concentration contrast medium of 270 mg I/mL can still maintain the contrast enhancement in coronary arteries without impairing image quality and significantly lower the radiation dose.
Coronary computed tomography (CT) angiography (CCTA) is a reliable and accurate method for diagnosis or exclusion of coronary artery disease. A large number of studies have investigated the diagnostic performance of CCTA among different generations of CT scanners . Although the high image quality and diagnostic accuracy are generally acknowledged, radiation exposure is of concern in CCTA . In a multicenter multivendor trial, Hausleiter et al. showed a median effective radiation dose of 12 mSv for CCTA with retrospective electrocardiography (ECG) gating using different types of 64-slice CT. With the introduction of post–64-slice CT technology, more dose-reduction strategies have been used to reduce radiation dose.
Various strategies and efforts are available to reduce the radiation exposure associated with CCTA. Examples include anatomic and ECG-dependent tube current modulation, reduced tube voltage , prospective ECG-triggering technique , and high-pitch spiral acquisitions . Prospectively ECG-triggered high-pitch spiral acquisition, which uses pitch values of ≥3.0, avoids overlapping radiation exposure. It also has been demonstrated that for selected patients, the combination of prospectively ECG-triggered high-pitch acquisition with 100-kV tube voltage allows CCTA with a consistent effective dose of <1.0 mSv and high image quality . Another feasibility study by Schuhbaeck et al. even reported an average radiation dose of <0.1 mSv in a highly selected population (with body weight <100 kg, heart rate ≤60 beats per minute [bpm]) performed with a prospectively ECG-triggered high-pitch spiral acquisition mode with 80 kV and 50 mAs.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Materials and methods
Study Population
Get Radiology Tree app to read full this article<
CT Acquisition and Image Reconstruction
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Image Quality of Coronary Artery Segments
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Measurement of Radiation Dose
Get Radiology Tree app to read full this article<
Evaluation of Adverse Effects Due to Contrast Medium
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Results
Study Population
Get Radiology Tree app to read full this article<
Table 1
Patient Demographics and Characteristics Overall and of the Two Groups
Demographics and Characteristics Overall Iodixanol 270 Iopromide 370 Total no. (men) 100 50 50 Age (years) 54.36 ± 9.82 55.14 ± 9.44 53.58 ± 10.23 Gender (M/F) 63/37 35/15 28/22 Body weight (kg) 62.99 ± 8.78 62.27 ± 8.99 63.71 ± 8.60 Body height (cm) 167.24 ± 7.26 167.00 ± 7.56 167.48 ± 6.91 BMI (kg/m 2 ) 22.44 ± 2.08 22.24 ± 2.10 22.63 ± 2.07 Heart rate (beats per minute) 57.21 ± 5.57 58.02 ± 6.53 56.40 ± 4.31 Tube potential (kVp) — 80 100 Reference tube current (mAs) 300 300 300 Effect tube current (mAs) 222.20 ± 42.66 218.74 ± 47.65 225.66 ± 37.19 Reconstruction algorithm — SAFIRE FBP
BMI, body mass index; F, female; FBP, filtered back projection; M, male; SAFIR, an iterative reconstruction product of Siemens Healthcare.
The values are means ± standard deviations.
Get Radiology Tree app to read full this article<
Subjective Image Quality
Get Radiology Tree app to read full this article<
Table 2
Image Quality Score and Percentage
Score Iodixanol 270 + 80 kV + SAFIRE, n (%) Iopromide 370 + 100 kV + FBP, n (%)P Value 1 332 (51.3) 352 (52.9) .577 2 237 (36.7) 251 (37.7) .651 3 74 (11.4) 61 (9.1) .174 4 4 (0.6) 2 (0.3) .393 1–3 643 (99.4) 664 (99.7) .393
FBP, filtered back projection; SAFIR, an iterative reconstruction product of Siemens Healthcare.
The value is presented as the number of segments (%).
![Figure 2, Two examples of curved planar reformation images of three coronary arteries obtained during the administration of two types of contrast medium. (a–c) shows right coronary artery (RCA), left anterior descending artery (LAD), and left circumflex artery (LCX) in a 43-year-old man (heart rate, 53 bpm; body mass index [BMI], 21.7 kg/m 2 ) who was administrated with 69 mL of Iodixanol 270, and the scan protocol was 80 kV and 300 mAs. (d–f) shows RCA, LAD, and LCX in a 50-year-old woman (heart rate, 53 bpm; BMI, 22.6 kg/m 2 ) who was administrated with 60 mL of iopromide 370, and the scan protocol was 100 kV and 300 mAs. Images from two patients show excellent and homogeneous arterial enhancement without visualized differences, and the image quality score was both 1 (excellent).](https://storage.googleapis.com/dl.dentistrykey.com/clinical/LowConcentrationContrastMediumfor128SliceDualSourceCTCoronaryAngiographyataVeryLowRadiationDoseUsingProspectivelyECGTriggeredHighPitchSpiralAcquisition/1_1s20S1076633214003687.jpg)
Get Radiology Tree app to read full this article<
Contrast Enhancement in the Coronary Arteries and Other Anatomic Regions
Get Radiology Tree app to read full this article<
Table 3
Attenuation and Noise in the Coronary Arteries and Other Anatomic Regions
Regions of Interest Iodixanol 270 + 80 kV + SAFIRE Iopromide 370 + 100 kV + FBP_P_ Value CT values Origin of the RCA (HU) 596.91 ± 70.22 564.44 ± 95.07 .057 Origin of the LCA (HU) 593.80 ± 76.05 561.57 ± 99.44 .065 Proximal ascending aorta (HU) 589.13 ± 59.60 561.01 ± 80.84 .053 Distal thoracic aorta (HU) 587.17 ± 51.32 559.65 ± 93.05 .063 Image noise Origin of the RCA 29.88 ± 5.25 28.24 ± 4.90 .110 Origin of the LCA 29.12 ± 4.89 27.52 ± 5.96 .146 Proximal ascending aorta 30.09 ± 3.97 28.78 ± 4.42 .121 Distal thoracic aorta 31.16 ± 4.02 30.33 ± 4.95 .305
CT, computed tomography; FBP, filtered back projection; HU, Hounsfield unit; LCA, left coronary artery; RCA, right coronary artery; SAFIR, an iterative reconstruction product of Siemens Healthcare.
The numbers are means ± standard deviations.
Get Radiology Tree app to read full this article<
Objective Image Quality
Get Radiology Tree app to read full this article<
Radiation Dose Estimation
Get Radiology Tree app to read full this article<
Table 4
Radiation Dose Measurements
Item Iodixanol 270 + 80 kV + SAFIRE Iopromide 370 + 100 kV + FBP_P_ Value CTDIvol (mGy) 0.97 ± 0.19 2.25 ± 0.42 .000 DLP (mGy.cm) 17.77 ± 3.43 40.87 ± 7.38 .000 Scan length (cm) 18.42 ± 0.82 18.29 ± 0.90 .581 Effective radiation dose (mSv) 0.26 ± 0.05 0.57 ± 0.10 .000
CTDI vol , volume computed tomography dose index; DLP, dose–length product; FBP, filtered back projection; SAFIR, an iterative reconstruction product of Siemens Healthcare.
Get Radiology Tree app to read full this article<
Adverse Effects with Injection of Contrast Material
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Study Limitations
Get Radiology Tree app to read full this article<
Acknowledgments
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Stein P.D., Beemath A., Kayali F., et. al.: Multidetector computed tomography for the diagnosis of coronary artery disease: a systematic review. Am J Med 2006; 119: pp. 203-216.
2. Einstein A.J., Henzlova M.J., Rajagopalan S.: Estimating risk of cancer associated with radiation exposure from 64-slice computed tomography coronary angiography. JAMA 2007; 298: pp. 317-323.
3. Hausleiter J., Meyer T., Hermann F., et. al.: Estimated radiation dose associated with cardiac CT angiography. JAMA 2009; 301: pp. 500-507.
4. Henzler T., Hanley M., Arnoldi E., et. al.: Practical strategies for low radiation dose cardiac computed tomography. J Thorac Imaging 2010; 25: pp. 213-220.
5. Hausleiter J., Meyer T., Hadamitzky M., et. al.: Radiation dose estimates from cardiac multislice computed tomography in daily practice: impact of different scanning protocols on effective dose estimates. Circulation 2006; 113: pp. 1305-1310.
6. Leschka S., Stolzmann P., Schmid F.T., et. al.: Low kilovoltage cardiac dual-source CT: attenuation, noise, and radiation dose. Eur Radiol 2008; 18: pp. 1809-1817.
7. d’Agostino A.G., Remy-Jardin M., Khalil C., et. al.: Low-dose ECG-gated 64-slices helical CT angiography of the chest: evaluation of image quality in 105 patients. Eur Radiol 2006; 16: pp. 2137-2146.
8. Earls J.P., Berman E.L., Urban B.A., et. al.: Prospectively gated transverse coronary CT angiography versus retrospectively gated helical technique: improved image quality and reduced radiation dose. Radiology 2008; 246: pp. 742-753.
9. Achenbach S., Marwan M., Ropers D., et. al.: Coronary computed tomography angiography with a consistent dose below 1 mSv using prospectively electrocardiogram-triggered high-pitch spiral acquisition. Eur Heart J 2010; 31: pp. 340-346.
10. Schuhbaeck A., Achenbach S., Layritz C., et. al.: Image quality of ultra-low radiation exposure coronary CT angiography with an effective dose <0.1 mSv using high-pitch spiral acquisition and raw data-based iterative reconstruction. Eur Radiol 2013; 23: pp. 597-606.
11. Nakazato R., Dey D., Gutstein A., et. al.: Coronary artery calcium scoring using a reduced tube voltage and radiation dose protocol with dual-source computed tomography. J Cardiovasc Comput Tomogr 2009; 3: pp. 394-400.
12. Huda W., Scalzetti E.M., Levin G.: Technique factors and image quality as functions of patient weight at abdominal CT. Radiology 2000; 217: pp. 430-435.
13. Marin D., Nelson R.C., Barnhart H., et. al.: Detection of pancreatic tumors, image quality, and radiation dose during the pancreatic parenchymal phase: effect of a low-tube-voltage, high-tube-current CT technique–preliminary results. Radiology 2010; 256: pp. 450-459.
14. Hou Y., Liu X., Xv S., et. al.: Comparisons of image quality and radiation dose between iterative reconstruction and filtered back projection reconstruction algorithms in 256-MDCT coronary angiography. AJR Am J Roentgenol 2012; 199: pp. 588-594.
15. Leipsic J., Labounty T.M., Heilbron B., et. al.: Estimated radiation dose reduction using adaptive statistical iterative reconstruction in coronary CT angiography: the ERASIR study. AJR Am J Roentgenol 2010; 195: pp. 655-660.
16. Wang R., Schoepf U.J., Wu R., et. al.: Image quality and radiation dose of low dose coronary CT angiography in obese patients: sinogram affirmed iterative reconstruction versus filtered back projection. Eur J Radiol 2012; 81: pp. 3141-3145.
17. Funama Y., Taguchi K., Utsunomiya D., et. al.: Combination of a low-tube-voltage technique with hybrid iterative reconstruction (iDose) algorithm at coronary computed tomographic angiography. J Comput Assist Tomogr 2011; 35: pp. 480-485.
18. Austen W.G., Edwards J.E., Frye R.L., et. al.: A reporting system on patients evaluated for coronary artery disease. Report of the Ad Hoc Committee for Grading of Coronary Artery Disease, Council on Cardiovascular Surgery, American Heart Association. Circulation 1975; 51: pp. 5-40.
19. Ghadri J.R., Kuiest S.M., Goetti R., et. al.: Image quality and radiation dose comparison of prospectively triggered low-dose CCTA: 128-slice dual-source high-pitch spiral versus 64-slice single-source sequential acquisition. Int J Cardiovasc Imaging 2012; 28: pp. 1217-1225.
20. Zhang C., Zhang Z., Yan Z., et. al.: 320-row CT coronary angiography: effect of 100-kV tube voltages on image quality, contrast volume, and radiation dose. Int J Cardiovasc Imaging 2011; 27: pp. 1059-1068.
21. McCollough C, Cody D, Edyvean S, et al AAPM report no. 96: the measurement, reporting, and management of radiation dose in CT—report of AAPM Task Group 23 of the Diagnostic Imaging Council CT Committee. American Association of Physicists in Medicine Website. http://www.aapm.Org/pubs/reports/RPT_96.pdf
22. Rutten A., Meijs M.F., de Vos A.M., et. al.: Biphasic contrast medium injection in cardiac CT: moderate versus high concentration contrast material at identical iodine flux and iodine dose. Eur Radiol 2010; 20: pp. 1917-1925.
23. Katzberg R.W., Barrett B.J.: Risk of iodinated contrast material–induced nephropathy with intravenous administration. Radiology 2007; 243: pp. 622-628.
24. Nyman U., Almen T., Aspelin P., et. al.: Contrast-medium-induced nephropathy correlated to the ratio between dose in gram iodine and estimated GFR in ml/min. Acta Radiol 2005; 46: pp. 830-842.
25. Cademartiri F., Mollet N.R., van der lugt A., et. al.: Intravenous contrast material administration at helical 16-detector row CT coronary angiography: effect of iodine concentration on vascular attenuation. Radiology 2005; 236: pp. 661-665.