
Rationale and Objectives
The aim of this study was to evaluate the effect of mean heart rate (HR) and HR variability on image quality in low-dose computed tomographic coronary angiography (CTCA) using prospective electrocardiographic (ECG) triggering.
Materials and Methods
One hundred thirty-six consecutive patients were scheduled for low-dose CTCA using prospective ECG triggering. The image quality of all coronary segments was rated on a 5-point scale by two independent readers (scores of 1–3 were considered diagnostic, and scores of 4 and 5 were considered nondiagnostic). Intravenous β blockers were administered targeting HR < 65 beats/min before scanning, but not if HR increased during scanning.
Results
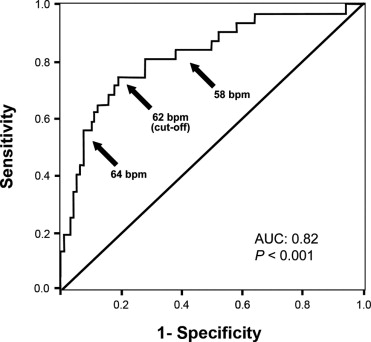
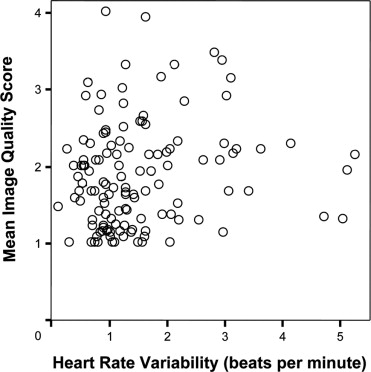
After the exclusion of seven patients because of arrhythmia ( n = 4) or mean HRs > 65 beats/min despite using β blockers ( n = 3), 129 patients underwent computed tomographic scanning. The estimated mean effective radiation dose was 2.2 ± 0.7 mSv (range, 1.1–3.5). The mean HR during scanning was 58.4 ± 6.6 beats/min (range, 44.2–80.1), with a variability of 1.6 ± 1.0 beats/min (range, 0.2–5.3). Mean HR ( r = 0.49, P < .001) but not mean HR variability ( r = 0.14) was related to image quality. Nondiagnostic image quality on CTCA was found in 5% of the coronary segments in 21 of 129 patients. However, on receiver-operating characteristic analysis, a cutoff HR of 62 beats/min was determined, below which nondiagnostic segments were significantly less frequent (2% vs 14%, P < .001).
Conclusion
Prospective triggering allows low-dose CTCA but requires a low HR. Because a low HR offers a prolonged diastole, widening the optimal phase for scanning, HR variability seems to have a negligible impact on image quality.
The implementation of multidetector computed tomography (MDCT) for coronary angiography allows fast imaging as well as increased temporal and spatial resolution ( ). However, motion artifacts caused by a higher heart rate (HR) or HR variability remain an issue, because they affect image quality. In four-slice and 16-slice MDCT, a higher HR has shown to cause a relevant degradation of image quality ( ). With 64-slice MDCT, the influence of HR and HR variability on image quality remains controversial, with such an effect reported by some authors ( ) but not by others ( ).
Despite further technical refinements and the introduction of dual-source computed tomographic (CT) coronary angiography (CTCA), leading to better temporal resolution, there still appears to be a negative influence of HR variability ( ) or both HR and HR variability ( ) on image quality. To minimize motion artifacts resulting from high HR or HR variability, images are usually reconstructed at the phase of near quiescence in mid-diastole called diastasis ( ). Scanning protocols using a spiral acquisition mode offer the opportunity for image reconstruction at any given point throughout the cardiac cycle, allowing the retrospective selection of any phase in the RR interval ( ) and the use of multisegment reconstructions for improving temporal resolution. With the introduction of prospective electrocardiographic (ECG) triggering ( ), radiation is administered at only one predefined time point in the cardiac cycle. This substantially reduces the effective radiation dose ( ) but in turn provides only a single data set for image reconstruction, achieving diagnostic image quality.
Get Radiology Tree app to read full this article<
Material and methods
Patients
Get Radiology Tree app to read full this article<
CT Data Acquisition and Postprocessing
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
CT Image Analysis
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Image Quality of Coronary Artery Segments
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
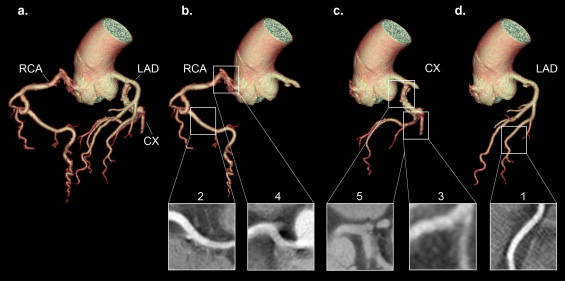
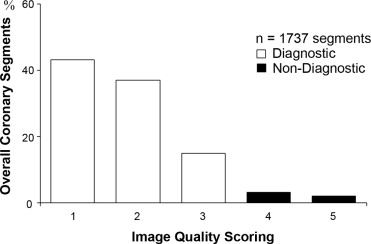
Table 1
Image Quality Scoring of All Segments
Coronary Artery Image Quality Score 1 2 3 4 5 ( n = 755) ( n = 635) ( n = 253) ( n = 56) ( n = 38) RCA Mean 176 173 107 23 11 Segment 1 50 50 16 9 3 Segment 2 22 32 55 12 7 Segment 3 51 44 27 2 1 Segment 4 53 47 9 0 0 LAD Mean 354 263 87 12 13 Segment 5 81 39 7 0 1 Segment 6 71 39 15 0 1 Segment 7 63 49 10 3 3 Segment 8 32 50 38 5 4 Segment 9 60 46 7 3 2 Segment 10 47 40 10 1 2 CX Mean 225 199 59 21 14 Segment 11 68 44 8 6 3 Segment 12 44 36 8 3 3 Segment 13 45 49 19 7 4 Segment 14 42 44 19 3 3 Segment 15 5 6 3 1 1 Segment 16 21 20 2 1 0
CX, circumflex coronary artery; LAD, left anterior descending coronary artery; RCA, right coronary artery.
Get Radiology Tree app to read full this article<
Impact of Mean HR on Image Quality
Get Radiology Tree app to read full this article<
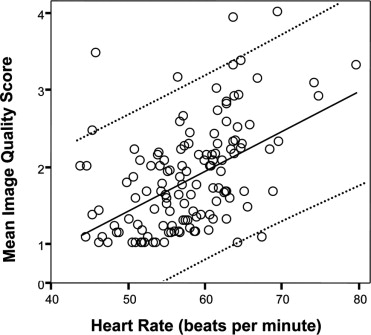
Table 2
Correlations
Image Score Mean HR Mean HR Variability_r__P__r__P_ All arteries 0.49 <.001 0.17 NS RCA 0.59 <.001 0.14 NS LAD 0.37 <.001 0.17 NS CX 0.37 <.001 0.10 NS
CX, circumflex coronary artery; HR, heart rate; LAD, left anterior descending coronary artery; NS, not significant; RCA, right coronary artery.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Impact of Mean HR Variability on Image Quality
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Brodoefel H., Burgstahler C., Tsiflikas I., et. al.: Dual-source CT: effect of heart rate, heart rate variability, and calcification on image quality and diagnostic accuracy. Radiology 2008; 247: pp. 346-355.
2. Ferencik M., Nomura C.H., Maurovich-Horvat P., et. al.: Quantitative parameters of image quality in 64-slice computed tomography angiography of the coronary arteries. Eur J Radiol 2006; 57: pp. 373-379.
3. Herzog C., Arning-Erb M., Zangos S., et. al.: Multi-detector row CT coronary angiography: influence of reconstruction technique and heart rate on image quality. Radiology 2006; 238: pp. 75-86.
4. Hoffmann M.H., Shi H., Manzke R., et. al.: Noninvasive coronary angiography with 16-detector row CT: effect of heart rate. Radiology 2005; 234: pp. 86-97.
5. Hong C., Becker C.R., Huber A., et. al.: ECG-gated reconstructed multi-detector row CT coronary angiography: effect of varying trigger delay on image quality. Radiology 2001; 220: pp. 712-717.
6. Husmann L., Schepis T., Scheffel H., et. al.: Comparison of diagnostic accuracy of 64-slice computed tomography coronary angiography in patients with low, intermediate, and high cardiovascular risk. Acad Radiol 2008; 15: pp. 452-461.
7. Leschka S., Husmann L., Desbiolles L.M., et. al.: Optimal image reconstruction intervals for non-invasive coronary angiography with 64-slice CT. Eur Radiol 2006; 16: pp. 1964-1972.
8. Matt D., Scheffel H., Leschka S., et. al.: Dual-source CT coronary angiography: image quality, mean heart rate, and heart rate variability. AJR Am J Roentgenol 2007; 189: pp. 567-573.
9. Leber A.W., Knez A., von Ziegler F., et. al.: Quantification of obstructive and nonobstructive coronary lesions by 64-slice computed tomography: a comparative study with quantitative coronary angiography and intravascular ultrasound. J Am Coll Cardiol 2005; 46: pp. 147-154.
10. Leschka S., Alkadhi H., Plass A., et. al.: Accuracy of MSCT coronary angiography with 64-slice technology: first experience. Eur Heart J 2005; 26: pp. 1482-1487.
11. Mollet N.R., Cademartiri F., van Mieghem C.A., et. al.: High-resolution spiral computed tomography coronary angiography in patients referred for diagnostic conventional coronary angiography. Circulation 2005; 112: pp. 2318-2323.
12. Pugliese F., Mollet N.R., Runza G., et. al.: Diagnostic accuracy of non-invasive 64-slice CT coronary angiography in patients with stable angina pectoris. Eur Radiol 2006; 16: pp. 575-582.
13. Raff G.L., Gallagher M.J., O’Neill W.W., Goldstein J.A.: Diagnostic accuracy of noninvasive coronary angiography using 64-slice spiral computed tomography. J Am Coll Cardiol 2005; 46: pp. 552-557.
14. Achenbach S., Ropers D., Holle J., Muschiol G., Daniel W.G., Moshage W.: In-plane coronary arterial motion velocity: measurement with electron-beam CT. Radiology 2000; 216: pp. 457-463.
15. Leschka S., Wildermuth S., Boehm T., et. al.: Noninvasive coronary angiography with 64-section CT: effect of average heart rate and heart rate variability on image quality. Radiology 2006; 241: pp. 378-385.
16. Lu B., Mao S.S., Zhuang N., et. al.: Coronary artery motion during the cardiac cycle and optimal ECG triggering for coronary artery imaging. Invest Radiol 2001; 36: pp. 250-256.
17. Manzke R., Kohler T., Nielsen T., Hawkes D., Grass M.: Automatic phase determination for retrospectively gated cardiac CT. Med Phys 2004; 31: pp. 3345-3362.
18. Mao S., Lu B., Oudiz R.J., Bakhsheshi H., Liu S.C., Budoff M.J.: Coronary artery motion in electron beam tomography. J Comput Assist Tomogr 2000; 24: pp. 253-258.
19. Vembar M., Garcia M.J., Heuscher D.J., et. al.: A dynamic approach to identifying desired physiological phases for cardiac imaging using multislice spiral CT. Med Phys 2003; 30: pp. 1683-1693.
20. Vembar M., Walker M.J., Johnson P.C.: Cardiac imaging using multislice computed tomography scanners: technical considerations. Coron Artery Dis 2006; 17: pp. 115-123.
21. Hsieh J., Londt J., Vass M., Li J., Tang X., Okerlund D.: Step-and-shoot data acquisition and reconstruction for cardiac x-ray computed tomography. Med Phys 2006; 33: pp. 4236-4248.
22. Husmann L., Valenta I., Gaemperli O., et. al.: Feasibility of low-dose coronary CT angiography: first experience with prospective ECG-gating. Eur Heart J 2008; 29: pp. 191-197.
23. Einstein A.J., Moser K.W., Thompson R.C., Cerqueira M.D., Henzlova M.J.: Radiation dose to patients from cardiac diagnostic imaging. Circulation 2007; 116: pp. 1290-1305.
24. Austen W.G., Edwards J.E., Frye R.L., et. al.: A reporting system on patients evaluated for coronary artery disease. Circulation 1975; 51: pp. 5-40.
25. Martuscelli E., Romagnoli A., D’Eliseo A., et. al.: Accuracy of thin-slice computed tomography in the detection of coronary stenoses. Eur Heart J 2004; 25: pp. 1043-1048.
26. Rybicki F.J., Otero H.J., Steigner M.L., et. al.: Initial evaluation of coronary images from 320-detector row computed tomography. Int J Cardiovasc Imaging 2008; 24: pp. 535-546.
27. Einstein A.J., Henzlova M.J., Rajagopalan S.: Estimating risk of cancer associated with radiation exposure from 64-slice computed tomography coronary angiography. JAMA 2007; 298: pp. 317-323.
28. Earls J.P., Berman E.L., Urban B.A., et. al.: Prospectively gated transverse coronary CT angiography versus retrospectively gated helical technique: improved image quality and reduced radiation dose. Radiology 2008; 246: pp. 742-753.
29. Chung C.S., Karamanoglu M., Kovacs S.J.: Duration of diastole and its phases as a function of heart rate during supine bicycle exercise. Am J Physiol Heart Circ Physiol 2004; 287: pp. H2003-H2008.
30. Kovacs S.J.: The duration of the QT interval as a function of heart rate: a derivation based on physical principles and a comparison to measured values. Am Heart J 1985; 110: pp. 872-878.
31. Wintersperger B.J., Nikolaou K., von Ziegler F., et. al.: Image quality, motion artifacts, and reconstruction timing of 64-slice coronary computed tomography angiography with 0.33-second rotation speed. Invest Radiol 2006; 41: pp. 436-442.
32. Dewey M., Muller M., Eddicks S., et. al.: Evaluation of global and regional left ventricular function with 16-slice computed tomography, biplane cineventriculography, and two-dimensional transthoracic echocardiography: comparison with magnetic resonance imaging. J Am Coll Cardiol 2006; 48: pp. 2034-2044.
33. Schepis T., Gaemperli O., Koepfli P., et. al.: Comparison of 64-slice CT with gated SPECT for evaluation of left ventricular function. J Nucl Med 2006; 47: pp. 1288-1294.