
Rationale and Objectives
Implementation of low dose computed tomography (LDCT) lung cancer screening programs has followed the demonstration of reduced lung cancer mortality in the National Lung Screening Trial and subsequent consensus screening recommendations. Here we aim to assess the initial results of a screening program at an academic medical center, to discuss the challenges of implementing such a program, and suggest strategies for reducing patient dose.
Materials and Methods
Retrospective review of all patients who underwent LDCT lung cancer screening at our institution between March 2015 and July 2016 was performed to assess the lung cancer detection rate, the spectrum of imaging findings (nodule or mass characteristics, degree of emphysema, etc.), and patient radiation dose indices.
Results
A total of 272 patients were screened during the study period. Approximately 50% ( n = 135) were women. The lung cancer detection rate was 2.2% ( n = 6). One patient underwent chemoradiation therapy, whereas the remainder underwent uneventful thoracoscopic resection. Approximately, 80% of screened patients met United States Preventative Services Task Force criteria for LDCT screening. The median pack-years of smoking was 42 pack-years. The mean volume CT dose index for the screening CTs was 3.12 mGy. Utilizing tube current modulation and iterative reconstruction, where available, resulted in lower patient doses.
Conclusion
Initial LDCT lung cancer screening at our institution yielded results similar to those of the National Lung Screening Trial. Thorough prescreening evaluation, joint decision-making, centralized coordination of screening-related care, and patient size conscious scanning protocols are critical elements of a safe and successful lung cancer screening program.
Introduction
Lung cancer is the leading cause of cancer death worldwide, accounting for an estimated 13% of new cancer diagnoses and 27% of all cancer deaths . Despite advances in medical and surgical intervention and imaging techniques, the overall 5-year survival rate for those diagnosed with lung or bronchial cancer is 17.8%, largely in part due to the advanced stage at diagnosis .
The development of effective lung cancer screening tools has remained challenging. Early studies of computed tomography (CT) demonstrated increased sensitivity for detecting lung cancer, but single-arm design precluded assessment of mortality benefit . The National Lung Cancer Screening Trial (NLST) demonstrated that lung cancer screening using low-dose computed tomography (LDCT) not only detected more nodules and cancers than conventional chest radiography, but that disease was discovered at an earlier stage than with conventional chest radiography, providing a survival benefit with 20% reduction in lung cancer-related mortality .
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Materials and Methods
Study Population
Get Radiology Tree app to read full this article<
Computed Tomography Scan Acquisition
Get Radiology Tree app to read full this article<
Data Abstraction
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Results
Patient Characteristics
Get Radiology Tree app to read full this article<
Table 1
Baseline Characteristics of the Screened Cohort
Demographic Mean age 64 (range 29–82) Sex Female 135 (50%) Male 137 (50%) Mean smoking duration (pack-years) 42 History of malignancy \* Yes 56 (21%) No 216 (79%) Met USPSTF screening criteria Yes 218 (80%) No 54 (20%)
USPSTF, United States Preventive Services Task Force.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Clinical Findings
Get Radiology Tree app to read full this article<
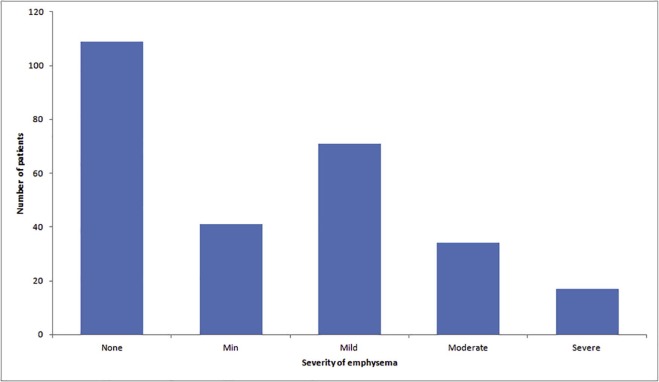
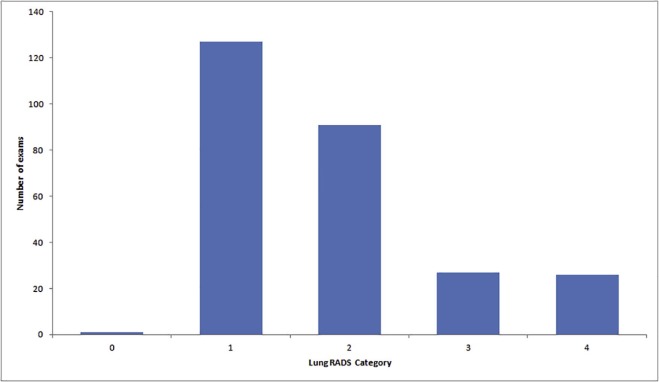
Table 2
LDCT Screening Findings
Parameter_n_ (%) Comparison CT Yes 69 (25) No 203 (75) Mean number of nodules 0.83 (range 0–8) Degree of emphysema None 109 (40) Minimal 41 (15) Mild 71 (26) Moderate 34 (13) Severe 17 (6) Lymphadenopathy Yes 18 (7) No 254 (93) Lung-RADS score 0 1 (0.4) 1 127 (46.7) 2 91 (33.4) 3 27 (9.9) 4 26 (9.6)
CT, computed tomography; RADS, Reporting and Data System.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 3
Screen Detected Lung Cancer
Case Location LAD by CT Positive Nodes at Biopsy or Surgery Pathology TNM Stage (At Biopsy or Surgery) Treatment 1 RUL No No Adenocarcinoma T1aN0M0 Thoracoscopic right upper lobectomy 2 LUL Yes Yes Adenocarcinoma T2aN2M0 Partial neoadjuvant chemotherapy + thoracoscopic left upper lobectomy 3 Right hilar Yes Yes Small cell lung cancer T3N2M1b Palliative chemoradiation 4 RLL No No Adenocarcinoma T1bN0M0 Thoracoscopic right lower lobectomy 5 RLL Yes (stable from comparison) No Squamous cell carcinoma T2aN0M0 Thoracoscopic right lower lobectomy 6 RUL Yes (partially calcified) No Adenocarcinoma T2aN0M0 Thoracoscopic right upper lobectomy
CT, computed tomography; LAD, lymphadenopathy; LUL, left upper lobe; RLL, right lower lobe; RUL, right upper lobe.

Get Radiology Tree app to read full this article<
CT Scanners and Dose Metrics
Get Radiology Tree app to read full this article<
Table 4
CT Scanners Utilized for Lung Cancer Screening
CT Scanner Number of Patients Examined Phillips Forte 1 Siemens Sensation 16 226 Toshiba Aquilion 16 4 Toshiba Aquilion 64 4 Toshiba Aquilion ONE 5 Toshiba Aquilion PRIME 32
CT, computed tomography.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Limitations
Get Radiology Tree app to read full this article<
Conclusion
Get Radiology Tree app to read full this article<
References
1. American Cancer Society : Cancer facts & figures.2015.American Cancer SocietyAtlanta, GApp. 2015.
2. Howlader N.Noone A.M.Krapcho M. et. al.SEER cancer statistics review, 1975–2012.2015.National Cancer InstituteBethesda, MD: Available at http://seer.cancer.gov/csr/1975_2012/ Accessed April 6, 2017
3. Sobue T., Moriyama N., Kaneko M., et. al.: Screening for lung cancer with low-dose helical computed tomography: anti-lung cancer association project. J Clin Oncol 2002; 20: pp. 911-920.
4. Nawa T., Nakagawa T., Kusano S., et. al.: Lung cancer screening using low-dose spiral CT: results of baseline and 1-year follow-up studies. Chest 2002; 122: pp. 15-20.
5. Henschke C.I., Naidich D.P., Yankelevitz D.F., et. al.: Early lung cancer action project: initial findings on repeat screenings. Cancer 2001; 92: pp. 153-159.
6. Swensen S.J., Jett J.R., Hartman T.E., et. al.: CT screening for lung cancer: five-year prospective experience. Radiology 2005; 235: pp. 259-265.
7. Aberle D.R., Adams A.M., Berg C.D., et. al.: Reduced lung-cancer mortality with low-dose computed tomographic screening. N Engl J Med 2011; 365: pp. 395-409.
8. Moyer V.A.: Screening for lung cancer: U.S. Preventive Services Task Force recommendation statement. Ann Intern Med 2014; 160: pp. 330-338.
9. Centers for Medicare & Medicaid Services : Final National Coverage Determination on Screening for Lung Cancer with Low Dose Computed Tomography (LDCT) (CAG-00439N). February 52015.
10. Burnside E.S., Sickles E.A., Bassett L.W., et. al.: The ACR BIRADS experience: learning from history. J Am Coll Radiol 2009; 6: pp. 851-860.
11. ACR Lung Imaging Reporting and Data System (Lung-RADS). Available at http://www.acr.org/Quality-Safety/Resources/LungRADS
12. American Association of Physicists in Medicine : Lung Cancer Screening CT Protocols Version 4.0. http://www.aapm.org/pubs/CTProtocols/documents/LungCancerScreeningCT.pdf