
Objectives and Rationale
Medulloblastoma/primitive neuroectodermal tumor (MB/PNET) is the most common malignant tumor of the central nervous system (CNS) in children. MB/PNET survivors are at an increased risk for developing second malignancies. Little has been reported on development of low-grade lesions of the calvarium in the radiation field in MB/PNET survivors. The purpose of this study was to assess the frequency of the low-grade bone lesion development in the radiotherapy field in pediatric MB/PNET survivors and describe the imaging characteristics of these lesions.
Materials and Methods
Institutional review board approval was obtained for this retrospective review which was compliant with Health Insurance Portability and Accountability Act. Forty-one MB/PNET patients (29 male) who survived for at least 2 years after initiation of radiation therapy were included. The medical records were reviewed. The most recent available brain magnetic resonance imaging studies were evaluated.
Results
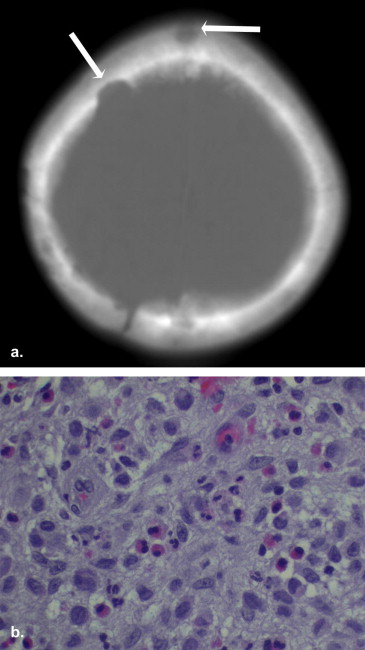
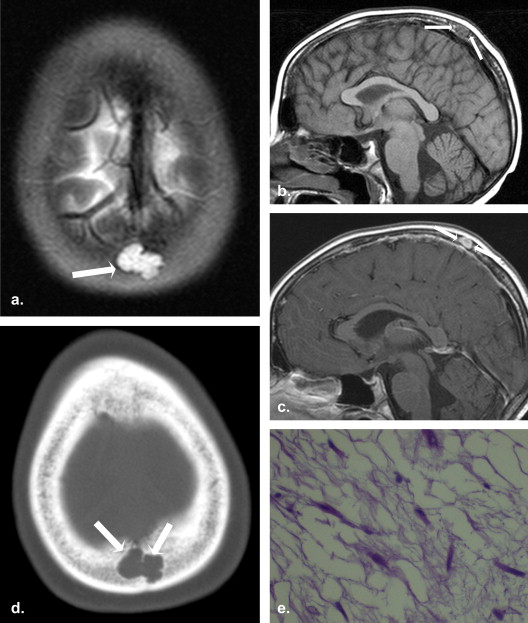
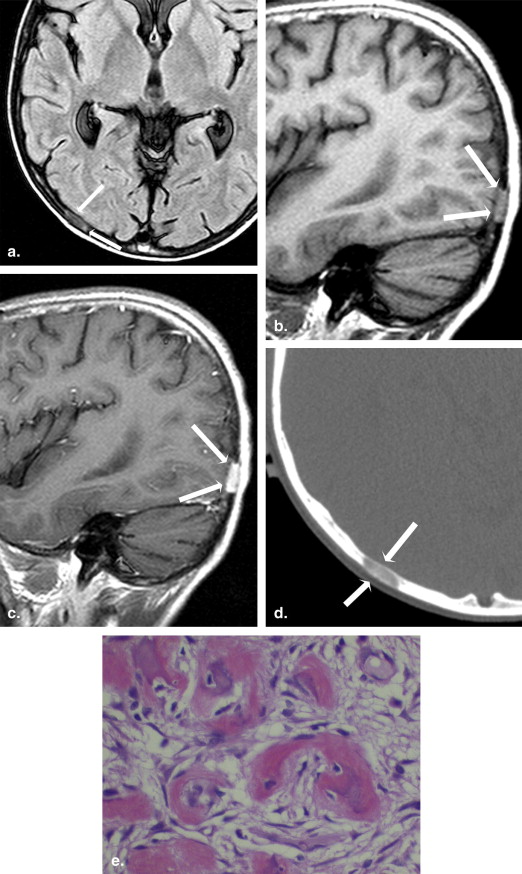
Three patients (7.3%) developed low-grade calvarial lesions and underwent resection and/or biopsy of the lesions. There were one Langerhans cell histiocytosis, one benign spindle cell lesion with myxoid change, and one fibrous dysplasia.
Conclusion
Development of low-grade bone lesions of calvarium is not very rare in pediatric PNET/MB survivors. Bones in the radiation therapy field need to be carefully examined for assessment of secondary lesions.
Medulloblastoma/primitive neuroectodermal tumor (MB/PNET) is the most common malignant brain tumor of childhood . With contemporary therapy, including surgical debulking, radiation therapy, and multiagent chemotherapy, current progression-free survival rates are up to 81% at 5 years . However, it is known that this impressive survival outcome is accompanied by many late therapy effects, including delay in cognitive functions, hormone deficiencies, growth impairment, second neoplasms, and strokes .
In addition to the late recurrence of the original neoplasm, the common second neoplasms reported among survivors of childhood MB/PNET include secondary leukemia, high-grade gliomas, meningiomas, and basal cell skin cancer . There are few data on the development of the low-grade skull lesions in the radiation therapy fields of pediatric MB/PNET survivors . The purpose of this study was to identify the frequency of low-grade skull lesions in the MB/PNET survivors at our institution and describe the imaging findings of these lesions.
Materials and methods
Patient Population
Get Radiology Tree app to read full this article<
Data Review
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Case 1
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Case 2
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Case 3
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. CBTRUS (2010). CBTRUS statistical report: primary brain and central nervous system tumors diagnosed in the United States in 2004–2006. Central Brain Tumor Registry of the United States, Hinsdale, IL. Available at: www.cbtrus.org . Accessed July 15, 2011.
2. Jakacki R.I.: Treatment strategies for high-risk medulloblastoma and supratentorial primitive neuroectodermal tumors. Review of the literature. J Neurosurg 2005; 102: pp. 44-52.
3. Packer R.J., Gajjar A., Vezina G., et. al.: Phase III study of craniospinal radiation therapy followed by adjuvant chemotherapy for newly diagnosed average-risk medulloblastoma. J Clin Oncol 2006; 24: pp. 4202-4208.
4. Armstrong G.T., Liu Q., Yasui Y., et. al.: Long-term outcomes among adult survivors of childhood central nervous system malignancies in the Childhood Cancer Survivor Study. J Natl Cancer Inst 2009; 101: pp. 946-958.
5. Morris E.B., Gajjar A., Okuma J.O., et. al.: Survival and late mortality in long-term survivors of pediatric CNS tumors. J Clin Oncol 2007; 25: pp. 1532-1538.
6. Neglia J.P., Robison L.L., Stovall M., et. al.: New primary neoplasms of the central nervous system in survivors of childhood cancer: a report from the Childhood Cancer Survivor Study. J Natl Cancer Inst 2006; 98: pp. 1528-1537.
7. Meadows A.T., Friedman D.L., Neglia J.P., et. al.: Second neoplasms in survivors of childhood cancer: findings from the Childhood Cancer Survivor Study cohort. J Clin Oncol 2009; 27: pp. 2356-2362.
8. Frange P., Alapetite C., Gaboriaud G., et. al.: From childhood to adulthood: long-term outcome of medulloblastoma patients. The Institut Curie experience (1980–2000). J Neurooncol 2009; 95: pp. 271-279.
9. Paling M.R., Herdt J.R.: Radiation osteitis: a problem of recognition. Radiology 1980; 137: pp. 339-342.
10. Campbell A.N., Chan H.S., Becker L.E., et. al.: Extracranial metastases in childhood primary intracranial tumors. A report of 21 cases and review of the literature. Cancer 1984; 53: pp. 974-981.
11. Algra P.R., Postma T., Van Groeningen C.J., et. al.: MR imaging of skeletal metastases from medulloblastoma. Skeletal Radiol 1992; 21: pp. 425-430.
12. Rochkind S., Blatt I., Sadeh M., et. al.: Extracranial metastases of medulloblastoma in adults: literature review. J Neurol Neurosurg Psychiatry 1991; 54: pp. 80-86.
13. Eberhart C.G., Cohen K.J., Tihan T., et. al.: Medulloblastomas with systemic metastases: evaluation of tumor histopathology and clinical behavior in 23 patients. J Pediatr Hematol Oncol 2003; 25: pp. 198-203.
14. Eberhart C.G., Kepner J.L., Goldthwaite P.T., et. al.: Histopathologic grading of medulloblastomas: a Pediatric Oncology Group study. Cancer 2002; 94: pp. 552-560.
15. Tabone M.D., Terrier P., Pacquement H., et. al.: Outcome of radiation-related osteosarcoma after treatment of childhood and adolescent cancer: a study of 23 cases. J Clin Oncol 1999; 17: pp. 2789-2795.
16. Bluemke D.A., Fishman E.K., Scott W.W., et. al.: Skeletal complications of radiation therapy. Radiographics 1994; 14: pp. 111-121.
17. Dalinka M.K., Mazzeo V.P.: Complications of radiation therapy. Crit Rev Diagn Imaging 1985; 23: pp. 235-267.
18. Murphy F.D., Blount W.P.: Cartilaginous exostoses following irradiation. J Jt Bone Surg 1962; 44: pp. 662-668.