
Rationale and Objectives
Pilot study to determine whether among subjects receiving coronary computed tomography angiography (CTA), the combination of high-sensitivity troponin I (hsTnI) and coronary artery calcium score (CACS) identifies a low-risk population in whom CTA might be avoided.
Materials and Methods
A cross-sectional study of 314 symptomatic patients receiving CTA as part of their acute coronary syndrome evaluation was conducted. hsTnI was measured with Abbott Laboratories’ hsTnI assay. CACSs were calculated via the Agatston method. Patients were followed for at least 30 days after discharge for the occurrence of major adverse cardiac events (MACEs; all-cause mortality, acute coronary syndrome, and revascularization).
Results
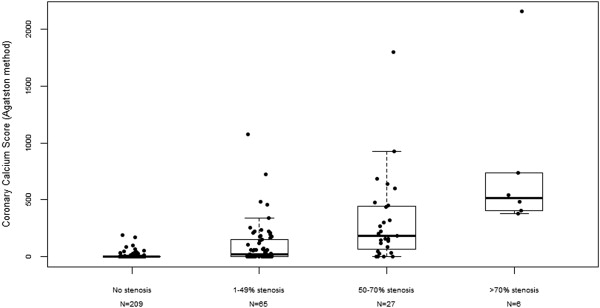
Of 314 subjects studied, 213 (67.8%) had no coronary artery stenosis, and 67 (21.3%), 28 (8.9%), and 6 (1.9%) had maximal coronary artery stenosis of 1%–49%, 50%–69%, and 70% or greater, respectively. All MACEs occurred during index hospitalization and include one myocardial infarction and four revascularizations. Sixty-two percent (189/307) of subjects had zero CACS, and 24% (76/314) of subjects had undetected hsTnI. No subjects with undetectable hsTnI or zero CACS had an MACE. A strategy of avoiding further testing in subjects with undetectable initial hsTnI, performing CACS on subjects with detectable initial hsTnI but nonincreased hsTnI (less than 99th percentile), and obtaining CTA in subjects with Agatston greater than 0 will have a negative predictive value of 100.0% (95% confidence interval, 98.2%–100.0%). This strategy will avoid CTA in 63% (198/314) of subjects.
Conclusions
In this pilot study, the addition of CACS to hsTnI improves the identification of low-risk subjects in whom CTA might be avoided.
Emergency Department (ED) evaluation of patients with suspected acute coronary syndromes (ACSs) is time consuming and costly . Many patients with symptoms suggestive of ACS, including low-risk patients, undergo extensive evaluation. Recently, coronary computed tomography angiography (CTA)-based strategies have been shown to identify suspected ACS patients who can be discharged expeditiously . However, CTA involves exposure to ionizing radiation and is costly if used indiscriminately .
A number of investigators have suggested that patients with suspected ACS who have zero coronary artery calcium score (CACS) might be a group that could be discharged home without the need for further diagnostic testing . However, in a pooled analysis of six studies a small number of patients with zero CACS had an adverse outcome. Of note, half of those with zero CACS and an adverse outcome had increased troponin measured by conventional assays .
Get Radiology Tree app to read full this article<
Methods
Study Design and Setting
Get Radiology Tree app to read full this article<
Selection of Participants
Get Radiology Tree app to read full this article<
Methods and Measurements
Get Radiology Tree app to read full this article<
Coronary CT Angiography
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Outcomes
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
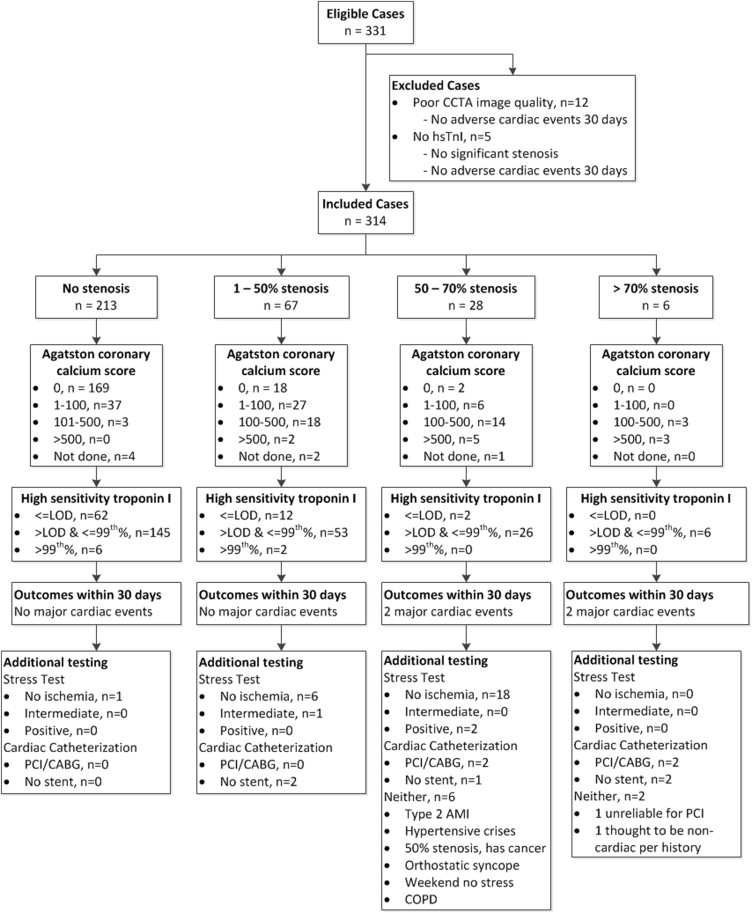
Table 1
Demographic Characteristics of Study Population ( n = 314)
Characteristic Number (%) Median age in years (interquartile range) 51.1 (45.5–58.5) Gender Female 177 (56.4) Male 137 (43.6) Ethnicity Non-Hispanic Black 218 (69.4) Non-Hispanic White 73 (23.2) Hispanic 7 (2.2) Asian 4 (1.3) Native-American 11 (3.5) Native-Hawaiian 1 (0.3) Insurance Medicare 55 (17.5) Medicaid 82 (26.1) Commercial 135 (43.0) HMO 10 (3.2) VA 3 (1.0) None 29 (9.2) Transportation Self-transport 259 (82.5) Ambulance 45 (14.3) Transfer from other facility 10 (3.2) Current cigarette smoker 131 (41.7) Current cocaine use 14 (4.5) Family history of AMI or sudden cardiac death 100 (31.8) History of hypertension 168 (53.5) History of diabetes 60 (19.1) History of high cholesterol 99 (31.5) History of congestive heart failure 10 (3.2) History of stroke 20 (6.4)
AMI, Acute Myocardial Infarction; HMO, Health Maintenance Organization; VA, Veterans Affairs.
Get Radiology Tree app to read full this article<
hsTnI and CACS Measurements
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Outcomes
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Using hsTnI Only to Define a Low-risk Population
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
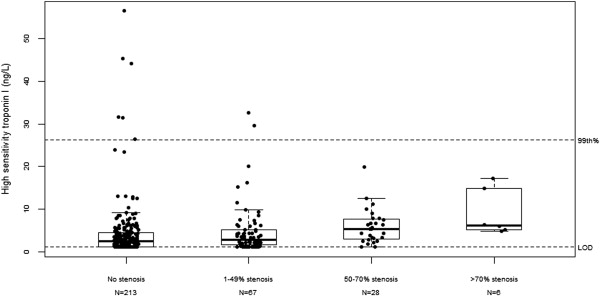
Table 2
Diagnostic accuracy Measures for Models Examined
Model Sensitivity (95% CI) Specificity (95% CI) PPV (95% CI) NPV (95% CI) Outcome: significant CAD (≥50% stenosis) CACS only 93.9 (79.8–99.3) 68.5 (62.6–74.0) 26.5 (18.8–35.4) 98.9 (96.2–99.9) HsTnI only 93.9 (79.8–99.3) 27.1 (21.9–32.7) 13.5 (9.3–18.6) 97.4 (90.8–99.7) HsTnI and CACS 100 (89.4–100) 22.0 (17.2–27.4) 13.4 (9.4–18.3) 100 (94.0–100) Outcome: major adverse cardiac event CACS >0 100 (47.8–100) 62.6 (56.9–68.1) 4.2 (1.4–9.6) 100 (98.1–100) HsTnI > LOD 100 (47.8–100) 25.2 (20.4–30.5) 2.2 (0.7–5.0) 100 (95.3–100) HsTnI >0 and CACS >0 100 (47.8–100) 19.4 (15.2–24.3) 2.0 (0.6–4.5) 100 (94.0–100)
CACS only, coronary artery calcium score only model recommends CTA for CACS >0; CAD, coronary artery disease; CI, confidence interval; CTA, coronary computed tomography angiography; HsTnI only, high-sensitivity troponin I only model recommends CTA for hsTnI > LOD; HsTnI and CACS, this model recommends CTA only in those with either hsTnI > LOD or CACS >0; LOD, limit of detection (1.2 ng/L); NPV, negative predictive value; PPV, positive predictive value.
Illustrative algorithm = initial testing with hsTnI, CACS in fourth quintile hsTnI, and CTA in CACS >0 or fifth quintile hsTnI.
Get Radiology Tree app to read full this article<
Using CACS Only to Define a Low-risk Population
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Combining hsTnI and CACS Values to Define a Low-risk Population
Get Radiology Tree app to read full this article<
Table 3
Diagnostic Strategies for Safely Avoiding CTAs
Diagnostic Evaluation Strategy CTAs Avoided Missed Significant CAD Missed MACE Measure hsTnI and CACS in all subjects and perform CTA in CACS >0 or detectable hsTnI 60 (19%) 0 0 Measure hsTnI in all subjects and perform CTA in subjects with detectable hsTnI 76 (24%) 2, All with negative nuclear stress test 0 Measure hsTnI in all subjects; measure CACS in subjects with detectable hsTnI and perform CTA in subjects with CACS >0 198 (63.1%) 4, All with negative nuclear stress tests 0
CACS, coronary artery calcium score; CTA, coronary computed tomography angiography; hsTnI, high-sensitivity troponin I; LOD, limit of detection (1.2 ng/L); MACE, major adverse cardiac event.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Limitations
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Conclusions
Get Radiology Tree app to read full this article<
Supplementary data
Get Radiology Tree app to read full this article<
Supplemental Table 1 and Legend for Supplemental Figure 1
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Bayley M.D., Schwartz J.S., Shofer F.S., et. al.: The financial burden of emergency department congestion and hospital crowding for chest pain patients awaiting admission. Ann Emerg Med 2005; 45: pp. 110-117.
2. Litt H.I., Gatsonis C., Snyder B., et. al.: CT angiography for safe discharge of patients with possible acute coronary syndromes. N Engl J Med 2012; 366: pp. 1393-1403.
3. Hoffmann U., Truong Q.A., Schoenfeld D.A., et. al.: Coronary CT angiography versus standard evaluation in acute chest pain. N Engl J Med 2012; 367: pp. 299-308.
4. Singer A.J., Poon M.: Coronary CT angiography reduces unnecessary admissions and allows safe discharge of emergency department patients with low-to-intermediate risk chest pain. Evid Based Med 2013; 18: pp. 64-65.
5. Nabi F., Chang S.M., Pratt C.M., et. al.: Coronary artery calcium scoring in the emergency department: identifying which patients with chest pain can be safely discharged home. Ann Emerg Med 2010; 56: pp. 220-229.
6. Laudon D.A., Behrenbeck T.R., Wood C.M., et. al.: Computed tomographic coronary artery calcium assessment for evaluating chest pain in the emergency department: long-term outcome of a prospective blind study. Mayo Clin Proc 2010; 85: pp. 314-322.
7. Laudon D.A., Vukov L.F., Breen J.F., et. al.: Use of electron-beam computed tomography in the evaluation of chest pain patients in the emergency department. Ann Emerg Med 1999; 33: pp. 15-21.
8. McLaughlin V.V., Balogh T., Rich S.: Utility of electron beam computed tomography to stratify patients presenting to the emergency room with chest pain. Am J Cardiol 1999; 84: pp. 327-328.
9. Hoffmann U., Bamberg F., Chae C.U., et. al.: Coronary computed tomography angiography for early triage of patients with acute chest pain: the ROMICAT (Rule Out Myocardial Infarction using Computer Assisted Tomography) trial. J Am Coll Cardiol 2009; 53: pp. 1642-1650.
10. Chang A.M., Le J., Matsuura A.C., et. al.: Does coronary artery calcium scoring add to the predictive value of coronary computed tomography angiography for adverse cardiovascular events in low-risk chest pain patients?. Acad Emerg Med 2011; 18: pp. 1065-1071.
11. Georgiou D., Budoff M.J., Kaufer E., et. al.: Screening patients with chest pain in the emergency department using electron beam tomography: a follow-up study. J Am Coll Cardiol 2001; 38: pp. 105-110.
12. Korley F.K., Schulman S.P., Sokoll L.J., et. al.: Troponin elevations only detected with a high-sensitivity assay: clinical correlations and prognostic significance. Acad Emerg Med 2014; 21: pp. 727-735.
13. Harris P.A., Taylor R., Thielke R., et. al.: Research electronic data capture (REDCap)—a metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform 2009; 42: pp. 377-381.
14. DeLong E.R., DeLong D.M., Clarke-Pearson D.L.: Comparing the areas under two or more correlated receiver operating characteristic curves: a nonparametric approach. Biometrics 1988; 44: pp. 837-845.
15. Pencina M.J., D’Agostino R.B., D’Agostino R.B., et. al.: Evaluating the added predictive ability of a new marker: from area under the ROC curve to reclassification and beyond. Stat Med 2008; 27: pp. 157-172.
16. Body R., Carley S., McDowell G., et. al.: Rapid exclusion of acute myocardial infarction in patients with undetectable troponin using a high-sensitivity assay. J Am Coll Cardiol 2011; 58: pp. 1332-1339.
17. Bandstein N., Ljung R., Johansson M., et. al.: Undetectable high sensitivity cardiac troponin T level in the emergency department and risk of myocardial infarction. J Am Coll Cardiol 2014; 63: pp. 2569-2578.
18. Apple F.S., Ler R., Murakami M.M.: Determination of 19 cardiac troponin I and T assay 99th percentile values from a common presumably healthy population. Clin Chem 2012; 58: pp. 1574-1581.
19. Rubini Giménez M., Hoeller R., Reichlin T., et. al.: Rapid rule out of acute myocardial infarction using undetectable levels of high-sensitivity cardiac troponin. Int J Cardiol 2013; 168: pp. 3896-3901.
20. Budoff M.J., Diamond G.A., Raggi P., et. al.: Continuous probabilistic prediction of angiographically significant coronary artery disease using electron beam tomography. Circulation 2002; 105: pp. 1791-1796.
21. Haberl R., Becker A., Leber A., et. al.: Correlation of coronary calcification and angiographically documented stenoses in patients with suspected coronary artery disease: results of 1,764 patients. J Am Coll Cardiol 2001; 37: pp. 451-457.
22. Pletcher M.J., Tice J.A., Pignone M., et. al.: Using the coronary artery calcium score to predict coronary heart disease events: a systematic review and meta-analysis. Arch Intern Med 2004; 164: pp. 1285-1292.
23. Tota-Maharaj R., McEvoy J.W., Blaha M.J., et. al.: Utility of coronary artery calcium scoring in the evaluation of patients with chest pain. Crit Pathw Cardiol 2012; 11: pp. 99-106.
24. Gottlieb I., Miller J.M., Arbab-Zadeh A., et. al.: The absence of coronary calcification does not exclude obstructive coronary artery disease or the need for revascularization in patients referred for conventional coronary angiography. J Am Coll Cardiol 2010; 55: pp. 627-634.
25. Heusch G., Kleinbongard P., Bose D., et. al.: Coronary microembolization: from bedside to bench and back to bedside. Circulation 2009; 120: pp. 1822-1836.
26. Mann J., Davies M.J.: Mechanisms of progression in native coronary artery disease: role of healed plaque disruption. Heart 1999; 82: pp. 265-268.
27. Ricciardi M.J., Wu E., Davidson C.J., et. al.: Visualization of discrete microinfarction after percutaneous coronary intervention associated with mild creatine kinase-MB elevation. Circulation 2001; 103: pp. 2780-2783.
28. Korosoglou G., Lehrke S., Mueller D., et. al.: Determinants of troponin release in patients with stable coronary artery disease: insights from CT angiography characteristics of atherosclerotic plaque. Heart 2011; 97: pp. 823-831.
29. Januzzi J.L., Bamberg F., Lee H., et. al.: High-sensitivity troponin T concentrations in acute chest pain patients evaluated with cardiac computed tomography. Circulation 2010; 121: pp. 1227-1234.
30. de Lemos J.A., Drazner M.H., Omland T., et. al.: Association of troponin T detected with a highly sensitive assay and cardiac structure and mortality risk in the general population. JAMA 2010; 304: pp. 2503-2512.
31. Polonsky T.S., McClelland R.L., Jorgensen N.W., et. al.: Coronary artery calcium score and risk classification for coronary heart disease prediction. JAMA 2010; 303: pp. 1610-1616.
32. Thygesen K., Alpert J.S., Jaffe A.S., et. al.: Third universal definition of myocardial infarction. J Am Coll Cardiol 2012; 60: pp. 1581-1598.
33. Hess E.P., Brison R.J., Perry J.J., et. al.: Development of a clinical prediction rule for 30-day cardiac events in emergency department patients with chest pain and possible acute coronary syndrome. Ann Emerg Med 2012; 59: pp. 115-125.
34. Maisel A., Mueller C., Neath S.X., et. al.: Copeptin helps in the early detection of patients with acute myocardial infarction: primary results of the CHOPIN trial (copeptin helps in the early detection of patients with acute myocardial infarction). J Am Coll Cardiol 2013; 62: pp. 150-160.
35. Than M., Herbert M., Flaws D., et. al.: What is an acceptable risk of major adverse cardiac event in chest pain patients soon after discharge from the Emergency Department?: A clinical survey. Int J Cardiol 2013; 166: pp. 752-754.