
Rationale and Objectives
To investigate the diagnostic performance of a comprehensive computed tomography (CT) protocol for both cardiac and aortoiliac evaluation of patients considered for transcatheter aortic valve replacement (TAVR) using a single, low-volume contrast medium (CM) injection.
Materials and Methods
Forty-four TAVR candidates were retrospectively analyzed. All underwent retrospectively electrocardiogram-gated cardiac CT followed by high-pitch CT angiography of the aortoiliac vasculature using one of two single injection protocols of 320 mgI/mL iodine CM: group A ( n = 22), iodine delivery rate-based (1.28 gI/s), 60-mL CM volume, 4.0 mL/s flow rate; group B ( n = 22), clinical routine protocol, 100-mL CM volume, 4.0 mL/s flow rate. Mean arterial attenuation, signal-to-noise ratio (SNR), and contrast-to-noise ratio (CNR) were calculated. Subjective image quality was assessed.
Results
Aortic root and iliofemoral dimensions could be analyzed in all cases. Patient characteristics showed no significant differences. Mean attenuation at the levels of the aortic root (285.8 ± 83.0 HU vs 327.5 ± 70.8 HU, P = .080) and the iliofemoral access route (256.8 ± 88.5 HU vs 307.5 ± 93.2 HU, P = .071), as well as SNR and CNR were nonsignificantly lower in group A compared to group B. Subjective image quality was equivalent.
Conclusions
In multimorbid TAVR patients, the performance of a combined CT protocol using a single low-volume CM bolus is feasible with maintained image quality compared to a standard protocol.
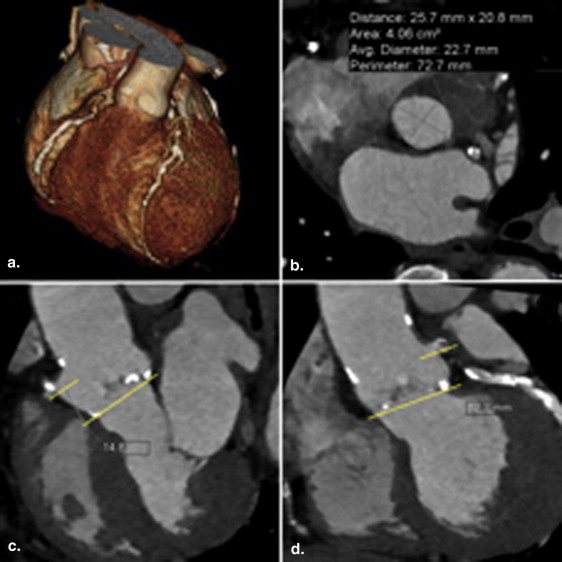
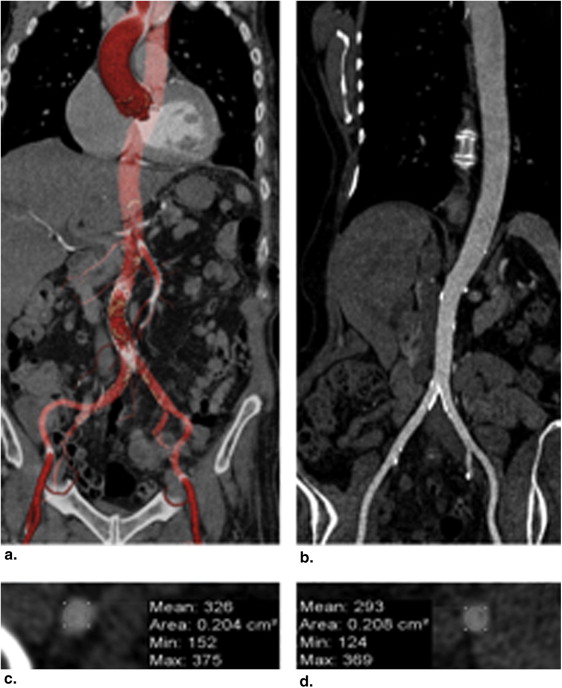
Transcatheter aortic valve replacement (TAVR) is an emerging minimally invasive procedure for patients with severe aortic valve stenosis who are considered at high risk for surgical treatment . A comprehensive preprocedural diagnostic work-up is essential for patient selection and proper TAVR planning . In this context, computed tomography (CT) is increasingly gaining importance as it provides information on both aortic annular sizing for prosthesis deployment and the aortoiliac access route within a single examination . Compared to other imaging modalities, CT offers this information noninvasively with three-dimensional reconstructions possible and without interference by overlaying structures. However, CT protocols of multiple body regions typically require a considerable amount of contrast medium (CM) using a conventional single-source CT system .
While designing an optimal CT protocol for TAVR planning, it is important to consider three frequent comorbid conditions in patients considered for TAVR: atrial fibrillation, heart failure, and chronic renal dysfunction , as they have both technical and clinical implications. Atrial fibrillation is important in that it might lead to incorrect aortic root measurements caused by cardiac motion and electrocardiogram (ECG) misregistration. This can be ameliorated by using a retrospectively ECG-gated image acquisition mode, which can also account for the conformational changes of the aortic annulus over the cardiac cycle that influence prosthesis sizing . Congestive heart failure and renal insufficiency together increase the risk of volume overload and renal compromise. Therefore, minimizing CM volume is desirable .
Get Radiology Tree app to read full this article<
Materials and methods
Patients
Get Radiology Tree app to read full this article<
CM Injection Protocol
Get Radiology Tree app to read full this article<
Table 1
CT Protocol for Combined Assessment of the Aortic Root Complex and the Aortoiliac access Route in TAVR Candidates
Parameter Heart Aortoiliac Vasculature CT protocol Tube voltage (kV) Adaptive Adaptive Tube current (modulated), mAs ref 500 500 Collimation 2 × 64 × 0.6 2 × 64 × 0.6 Rotation time (ms) 280 280 Pitch Heart rate adaptive 3.2 Study range Tracheal bifurcation to bottom of heart Lung apices to femoral heads Acquisition direction Caudocranial Craniocaudal ECG synchronization Retrospective Prospective Target R-R interval for data acquisition 0%–100% 35% Injection protocol Bolus timing Bolus tracking: threshold 100 HU, ROI in descending aorta (at the level of the bottom of the heart) Delay (s) 2 s (after threshold) 4 s (delay after cardiac study) Total CM volume (mL) 60 Flow rate (mL/s) 4.0 Image reconstruction (basic reconstructions) Aortic root complex Aortoiliac access route Section thickness (mm) 0.75 1.5 Increment (mm) 0.4 0.7 Kernel B26f B30f Reconstruction window 300 ms (absolute forward) 35% (single heart beat) Multiplanar reformation Sagittal, coronal: 2 mm
CM, contrast medium; CT, computed tomography; ECG, electrocardiogram; ROI, region of interest; TAVR, transcatheter aortic valve replacement.

Get Radiology Tree app to read full this article<
CT Protocol
Get Radiology Tree app to read full this article<
Image Reconstruction
Get Radiology Tree app to read full this article<
Qualitative Image Assessment
Get Radiology Tree app to read full this article<
Quantitative Assessment of IQ
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
SNR=HUvessel/noise SNR
=
HU
vessel
/
noise
CNR=(HUvessel−HUmuscle)/noise CNR
=
(
HU
vessel
−
HU
muscle
)
/
noise
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Radiation Dose
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Results
Demographics
Get Radiology Tree app to read full this article<
Qualitative Image Assessment
Get Radiology Tree app to read full this article<
Quantitative Assessment of IQ
Get Radiology Tree app to read full this article<
Table 2
Assessment of Objective Image Parameters
Parameter Attenuation (HU) SNR CNR Group A Group B_P_ Value Group A Group B_P_ Value Group A Group B_P_ Value Summary scores Cardiac 285.8 ± 83.0 327.5 ± 70.8 .080 16.3 ± 7.2 16.9 ± 5.3 .760 13.8 ± 6.6 14.4 ± 4.9 .664 Access route234.2 ± 79.1290.8 ± 95.0.038* 8.4 ± 3.4 11.1 ± 5.8 .069 6.7 ± 3.2 9.4 ± 5.3 .055 Aorta207.1 ± 71.5270.6 ± 105.8.024* 7.9 ± 3.6 11.3 ± 7.4 .0606.1 ± 3.39.4 ± 6.8.043* Iliac arteries 256.8 ± 88.5 307.5 ± 93.2 .071 8.9 ± 3.6 10.9 ± 4.9 .123 6.1 ± 3.3 9.4 ± 6.8 .109 Cardiac levels Pulmonary artery162.8 ± 76.8253.0 ± 128.6.007*9.0 ± 5.014.0 ± 7.9.038*6.4 ± 4.711.3 ± 8.6.030* Left ventricle 311.1 ± 103.1 325.0 ± 75.0 .611 16.6 ± 9.5 16.2 ± 9.8 .703 14.9 ± 8.1 14.1 ± 7.9 .739 Aortic root 317.8 ± 106.5 340.9 ± 72.7 .407 15.7 ± 9.6 15.3 ± 6.0 .461 15.3 ± 9.2 13.7 ± 5.6 .492 Ascending aorta 315.3 ± 104.6 367.9 ± 71.9 .058 17.5 ± 9.6 21.8 ± 10.9 .550 15.6 ± 8.3 17.0 ± 6.2 .536 Descending aorta 322.1 ± 101.3 350.9 ± 74.7 .289 15.3 ± 7.4 17.7 ± 7.0 .928 16.4 ± 9.4 16.1 ± 6.2 .912 Aortoiliac levels Ascending aorta186.0 ± 63.1262.3 ± 114.8.010* 8.0 ± 4.2 12.4 ± 9.7 .0575.8 ± 3.510.2 ± 8.9.035* Aortic arch188.8 ± 64.0262.5 ± 108.7.010*7.8 ± 3.312.2 ± 9.3.042*5.7 ± 2.810.0 ± 8.5.033* Descending aorta (level 1)191.4 ± 69.5259.1 ± 108.1.018*7.8 ± 3.411.8 ± 8.4.045*5.7 ± 2.99.7 ± 7.6.025* Descending aorta (level 2) 221.7 ± 82.5 274.5 ± 107.7 .075 7.3 ± 4.0 9.5 ± 5.1 .104 5.9 ± 3.7 8.0 ± 4.6 .101 Descending aorta (level 3) 247.4 ± 91.7 294.8 ± 104.8 .118 8.8 ± 5.1 10.7 ± 6.1 .255 7.3 ± 4.8 9.2 ± 5.7 .234 Common iliac artery 245.9 ± 89.3 300.3 ± 103.9 .073 8.2 ± 4.0 9.8 ± 5.7 .267 6.6 ± 3.8 8.3 ± 5.3 .219 External iliac artery 244.5 ± 94.6 297.8 ± 97.9 .0918.2 ± 3.310.6 ± 4.6.048* 6.7 ± 3.2 8.9 ± 4.4 .059 Common femoral artery 268.3 ± 96.7 326.1 ± 88.5 .073 10.3 ± 4.1 12.3 ± 5.2 .170 8.6 ± 3.9 10.6 ± 4.8 .131
Mean attenuation was measured by using a region of interest analysis. Based on these values, signal-to-noise (SNR) and contrast-to-noise (CNR) ratios were calculated. Values were provided as mean and standard deviation. Significant differences were indicated by bold letters and asterisks.
Get Radiology Tree app to read full this article<
Radiation Dose
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Leon M.B., Smith C.R., Mack M., et. al.: Transcatheter aortic-valve implantation for aortic stenosis in patients who cannot undergo surgery. N Engl J Med 2010; 363: pp. 1597-1607.
2. Smith C.R., Leon M.B., Mack M.J., et. al.: Transcatheter versus surgical aortic-valve replacement in high-risk patients. N Engl J Med 2011; 364: pp. 2187-2198.
3. Leipsic J., Wood D., Manders D., et. al.: The evolving role of MDCT in transcatheter aortic valve replacement: a radiologists’ perspective. AJR Am J Roentgenol 2009; 193: pp. W214-W219.
4. Apfaltrer P., Schymik G., Reimer P., et. al.: Aortoiliac CT angiography for planning transcutaneous aortic valve implantation: aortic root anatomy and frequency of clinically significant incidental findings. AJR Am J Roentgenol 2012; 198: pp. 939-945.
5. Blanke P., Euringer W., Baumann T., et. al.: Combined assessment of aortic root anatomy and aortoiliac vasculature with dual-source CT as a screening tool in patients evaluated for transcatheter aortic valve implantation. AJR Am J Roentgenol 2010; 195: pp. 872-881.
6. Bae K.T.: Intravenous contrast medium administration and scan timing at CT: considerations and approaches. Radiology 2010; 256: pp. 32-61.
7. Faggiano P., Frattini S., Zilioli V., et. al.: Prevalence of comorbidities and associated cardiac diseases in patients with valve aortic stenosis. Potential implications for the decision-making process. Int J Cardiol 2012; 159: pp. 94-99.
8. Blanke P., Schoepf U.J., Leipsic J.A.: CT in transcatheter aortic valve replacement. Radiology 2013; 269: pp. 650-669.
9. Karlo C., Leschka S., Goetti R.P., et. al.: High-pitch dual-source CT angiography of the aortic valve-aortic root complex without ECG-synchronization. Eur Radiol 2011; 21: pp. 205-212.
10. Kempfert J., Van Linden A., Lehmkuhl L., et. al.: Aortic annulus sizing: echocardiographic vs. computed tomography derived measurements in comparison with direct surgical sizing. Eur J Cardiothorac Surg 2012; 42: pp. 627-633.
11. Goetti R., Feuchtner G., Stolzmann P., et. al.: High-pitch dual-source CT coronary angiography: systolic data acquisition at high heart rates. Eur Radiol 2010; 20: pp. 2565-2571.
12. Apfaltrer P., Henzler T., Blanke P., et. al.: Computed tomography for planning transcatheter aortic valve replacement. J Thorac Imaging 2013; 28: pp. 231-239.
13. Blanke P., Russe M., Leipsic J., et. al.: Conformational pulsatile changes of the aortic annulus: impact on prosthesis sizing by computed tomography for transcatheter aortic valve replacement. JACC Cardiovasc Interv 2012; 5: pp. 984-994.
14. Utsunomiya D., Oda S., Funama Y., et. al.: Comparison of standard- and low-tube voltage MDCT angiography in patients with peripheral arterial disease. Eur Radiol 2010; 20: pp. 2758-2765.
15. Pontana F., Duhamel A., Pagniez J., et. al.: Chest computed tomography using iterative reconstruction vs filtered back projection (Part 2): image quality of low-dose CT examinations in 80 patients. Eur Radiol 2011; 21: pp. 636-643.
16. Szucs-Farkas Z., Strautz T., Patak M.A., et. al.: Is body weight the most appropriate criterion to select patients eligible for low-dose pulmonary CT angiography? Analysis of objective and subjective image quality at 80 kVp in 100 patients. Eur Radiol 2009; 19: pp. 1914-1922.
17. European Commission: European guidelines on quality criteria for computed tomography. Report EUR 16262. Brussels, Belgium1999.
18. Bongartz G., Golding S.J., Jurik A.G., et. al.: European Guidelines for multislice computed tomography: funded by the European Commission, Contract number FIGM-CT2000-20078-CT-TIP. [updated 20 Apr 2013; cited 2011 June]March 2004. Available at: http://www.msct.eu/CT_Quality_Criteria.htm
19. Goetti R., Baumuller S., Feuchtner G., et. al.: High-pitch dual-source CT angiography of the thoracic and abdominal aorta: is simultaneous coronary artery assessment possible?. AJR Am J Roentgenol 2010; 194: pp. 938-944.
20. Iung B., Cachier A., Baron G., et. al.: Decision-making in elderly patients with severe aortic stenosis: why are so many denied surgery?. Eur Heart J 2005; 26: pp. 2714-2720.
21. Reynolds M.R., Magnuson E.A., Lei Y., et. al.: Health-related quality of life after transcatheter aortic valve replacement in inoperable patients with severe aortic stenosis. Circulation 2011; 124: pp. 1964-1972.
22. Reynolds M.R., Magnuson E.A., Wang K., et. al.: Health-related quality of life after transcatheter or surgical aortic valve replacement in high-risk patients with severe aortic stenosis: results from the PARTNER (Placement of AoRTic TraNscathetER Valve) Trial (Cohort A). J Am Coll Cardiol 2012; 60: pp. 548-558.
23. Lehmkuhl L.H., von Aspern K., Foldyna B., et. al.: Comparison of aortic root measurements in patients undergoing transapical aortic valve implantation (TA-AVI) using three-dimensional rotational angiography (3D-RA) and multislice computed tomography (MSCT): differences and variability. Int J Cardiovasc Imaging 2013; 29: pp. 417-424.
24. Giordana F., D’Ascenzo F., Nijhoff F., et. al.: Meta-analysis of predictors of all-cause mortality after transcatheter aortic valve implantation. Am J Cardiol 2014; 114: pp. 1447-1455.
25. Fleischmann D., Kamaya A.: Optimal vascular and parenchymal contrast enhancement: the current state of the art. Radiol Clin North Am 2009; 47: pp. 13-26.
26. Vahanian A., Alfieri O., Al-Attar N., et. al.: Transcatheter valve implantation for patients with aortic stenosis: a position statement from the European association of cardio-thoracic surgery (EACTS) and the European Society of Cardiology (ESC), in collaboration with the European Association of Percutaneous Cardiovascular Interventions (EAPCI). Eur Heart J 2008; 29: pp. 1463-1470.
27. Anderson S.W., Soto J.A., Lucey B.C., et. al.: Blunt trauma: feasibility and clinical utility of pelvic CT angiography performed with 64-detector row CT. Radiology 2008; 246: pp. 410-419.
28. Wuest W., Anders K., Schuhbaeck A., et. al.: Dual source multidetector CT-angiography before transcatheter aortic valve implantation (TAVI) using a high-pitch spiral acquisition mode. Eur Radiol 2012; 22: pp. 51-58.
29. Karaca M., Kirilmaz A., Oncel G., et. al.: Contrast-enhanced 64-slice computed tomography in detection and evaluation of anomalous coronary arteries. Tohoku J Exp Med 2007; 213: pp. 249-259.
30. Leber A.W., Knez A., Becker C., et. al.: Non-invasive intravenous coronary angiography using electron beam tomography and multislice computed tomography. Heart 2003; 89: pp. 633-639.
31. Holmquist F., Hansson K., Pasquariello F., et. al.: Minimizing contrast medium doses to diagnose pulmonary embolism with 80-kVp multidetector computed tomography in azotemic patients. Acta Radiol 2009; 50: pp. 181-193.
32. Nietlispach F., Leipsic J., Al-Bugami S., et. al.: CT of the ilio-femoral arteries using direct aortic contrast injection: proof of feasibility in patients screened towards percutaneous aortic valve replacement. Swiss Med Wkly 2009; 139: pp. 458-462.