
Rationale and Objective
Emphysema is characterized by airspace dilation, inflammation, and irregular deposition of elastin and collagen in the interstitium. Computed tomographic studies have reported that lung mass (LM) may be increased in smokers, a finding attributed to inflammatory and parenchymal remodeling processes observed on histopathology. We sought to examine the epidemiologic and clinical associations of LM in smokers.
Materials and Methods
Baseline epidemiologic, clinical, and computed tomography (CT) data (n = 8156) from smokers enrolled into the COPDGene Study were analyzed. LM was calculated from the CT scan. Changes in lung function at 5 years’ follow-up were available from 1623 subjects. Regression analysis was performed to assess for associations of LM with forced expiratory volume in 1 second (FEV 1 ) and FEV 1 decline.
Results
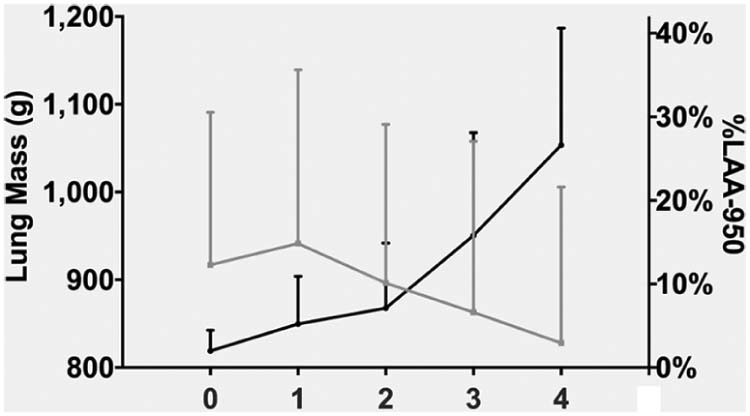
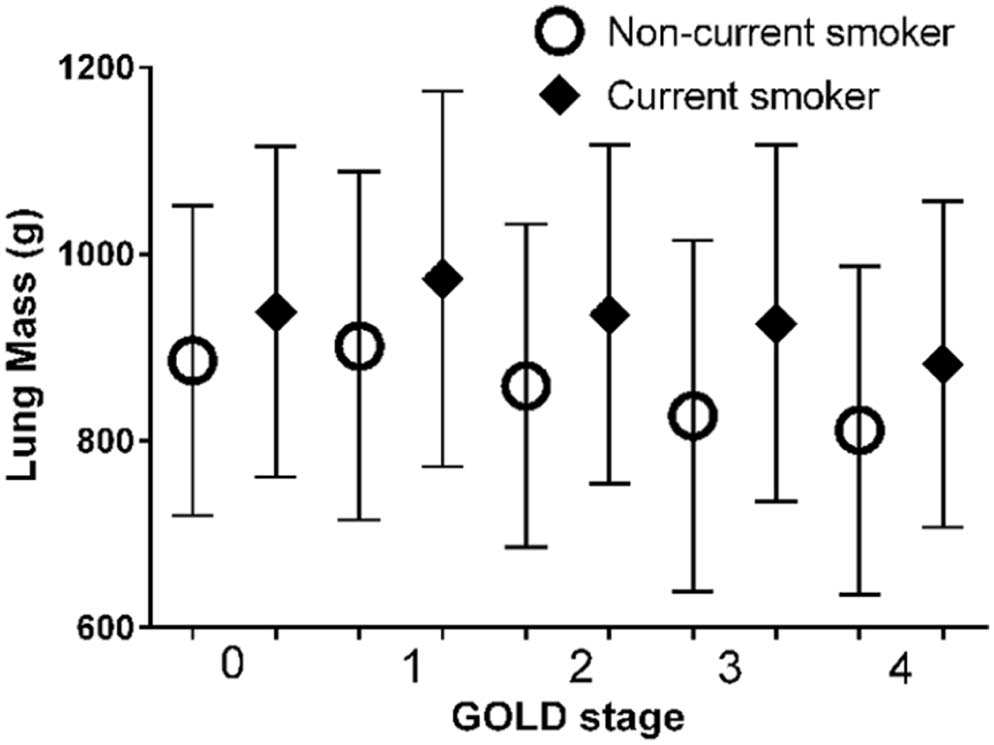
Subjects with Global Initiative for Chronic Obstructive Lung Disease (GOLD) 1 chronic obstructive pulmonary disease had greater LM than either smokers with normal lung function or those with GOLD 2–4 chronic obstructive pulmonary disease ( P < 0.001 for both comparisons). LM was predictive of the rate of the decline in FEV 1 (decline per 100 g, −4.7 ± 1.7 mL/y, P = 0.006).
Conclusions
Our cross-sectional data suggest the presence of a biphasic radiological remodeling process in smokers: the presence of such nonlinearity must be accounted for in longitudinal computed tomographic studies. Baseline LM predicts the decline in lung function.
Introduction
Emphysema is defined as an abnormal, permanent dilation of the distal airspaces . The development and progression of this pathologic process are associated with a decline in lung function and progressive clinical impairment . Spirometric measures of lung function have been the benchmark for monitoring progression of disease and response to therapeutic intervention, but such investigations lack sensitivity and require large cohorts followed over relatively long periods of time . For these reasons, computed tomographic imaging of the chest is increasingly being leveraged as a source of intermediate study end points to objectively assess response to treatment .
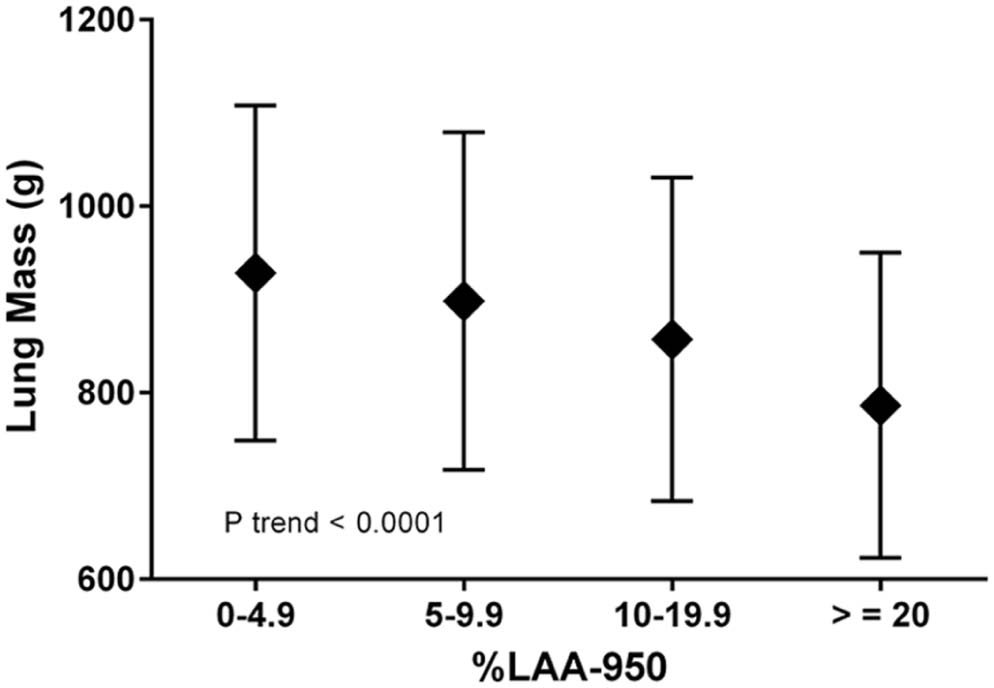
Densitometric measures of the lung parenchyma to detect and quantify emphysema have been utilized in cross-sectional investigations for almost 30 years , including the percent low-attenuation area (%LAA—those regions of the lung less than a select attenuation value) and the percentage of lung volume less than the 10th or 15th percentile . Each of these measures may have relative advantages when considering disease severity and progression but are all focused on the low-attenuation values of the lung histogram, the tail that may be most sensitive for the detection of airspace dilation. This may limit the ability of such metrics to fully assess the remodeling process characteristic of chronic obstructive pulmonary disease (COPD).
Get Radiology Tree app to read full this article<
Materials and Methods
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Spirometric Measurements and COPD Definition
Get Radiology Tree app to read full this article<
Clinical Assessment
Get Radiology Tree app to read full this article<
CT Assessment
Get Radiology Tree app to read full this article<
Lung mass(g)=HU+10241024∗Voxel volume∗No of voxels Lung mass
(
g
)
=
HU
+
1024
1024
∗
Voxel volume
∗
No of voxels
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
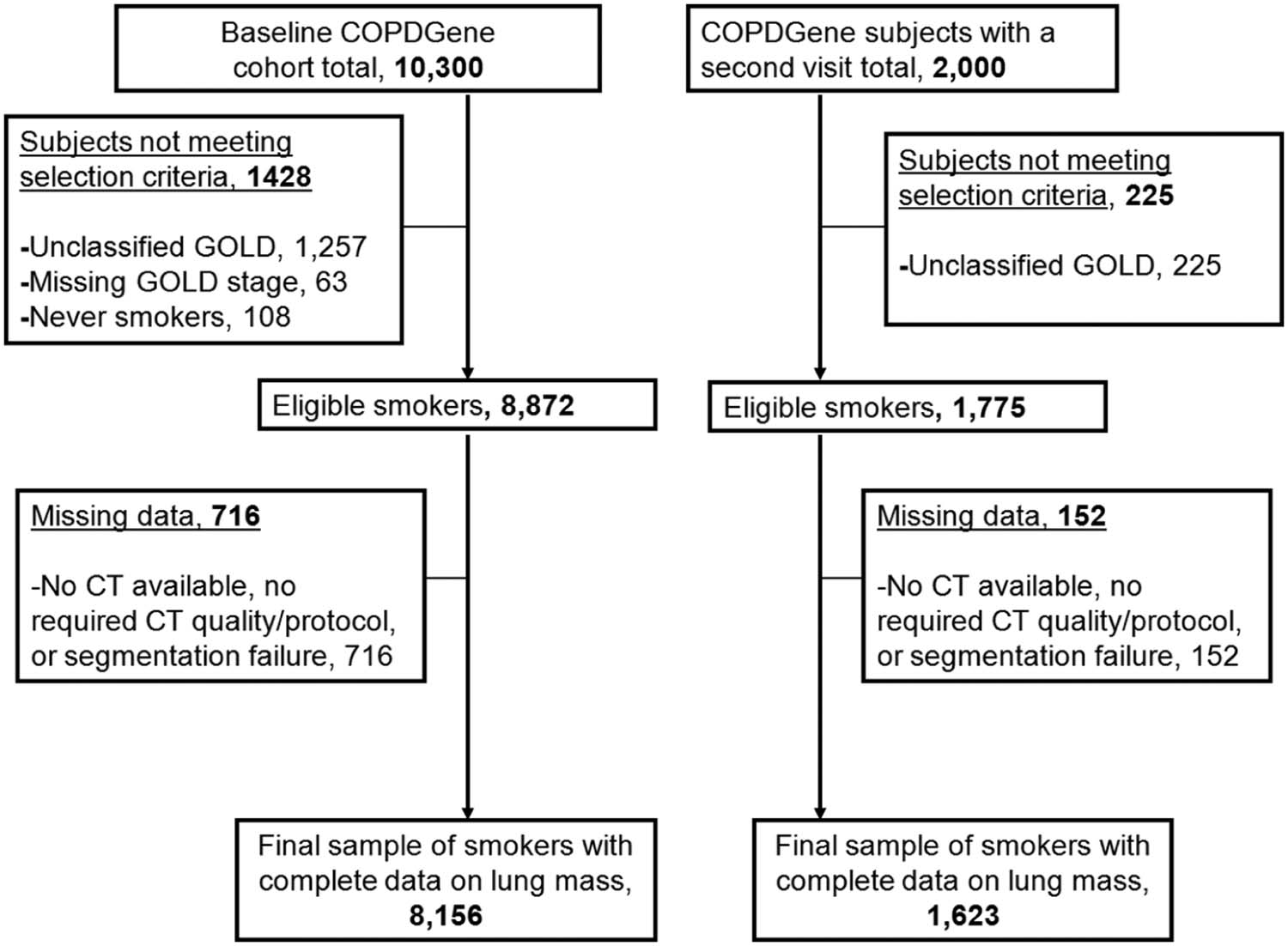
TABLE 1
Characteristics of the Subjects in the Baseline and of Those with a Second Visit
Characteristic Baseline ( N = 8156) Subjects with a Second Visit ( N = 1623) Age (y) 60 ± 9 61 ± 9 Male gender (%) 55 52 African-American race (%) 31 27 Height (cm) 170 ± 9 170 ± 9 Weight (kg) 82 ± 19 83 ± 18 Pack-years of smoking 44 ± 25 44 ± 24 Current smoking status (%) 51 43 FEV 1 (L) 2.3 ± 1.0 2.3 ± 0.9 FEV 1 change (mL/y) — −41 ± 52 FEV 1 (% predicted) 78 ± 27 80 ± 25 FVC (L) 3.4 ± 1.0 3.4 ± 1.0 FVC (% predicted) 89 ± 18 91 ± 17 FEV 1 /FVC ratio 0.65 ± 0.17 0.66 ± 0.16 %LAA-950 (%) 6.8 ± 10.0 7.1 ± 9.3 Lung mass (g) 902 ± 183 884 ± 174 Subjects with COPD (%) 50 50 One or more acute respiratory disease episodes in the prior year to enrollment (%) 21 18
COPD, chronic obstructive pulmonary disease; FEV 1 , forced expiratory volume in 1 second; FVC, forced vital capacity; %LAA, percent low-attenuation area.
Data are presented as mean ± standard deviation or proportion (%).
TABLE 2
Characteristics of the Subjects in the Baseline by GOLD Stage
Characteristic GOLD Stage 0 ( N = 4047) 1 ( N = 747) 2 ( N = 1786) 3 ( N = 1042) 4 ( N = 534) Age (y) 57 ± 8 62 ± 9 63 ± 9 64 ± 8 64 ± 8 Male gender (%) 53 58 54 58 59 African-American race (%) 41 22 24 20 18 Height (cm) 170 ± 9 170 ± 10 170 ± 9 170 ± 9 170 ± 9 Weight (kg) 84 ± 18 78 ± 16 83 ± 20 81 ± 20 73 ± 18 Pack-years of smoking 37 ± 20 45 ± 24 51 ± 27 55 ± 27 57 ± 29 Current smoking status (%) 59 55 49 36 23 FEV 1 (L) 2.9 ± 0.7 2.7 ± 0.7 1.9 ± 0.5 1.2 ± 0.3 0.7 ± 0.2 FEV 1 (% predicted) 98 ± 12 91 ± 9 65 ± 8 40 ± 6 23 ± 5 FVC (L) 3.7 ± 0.9 4.1 ± 1.0 3.2 ± 0.9 2.7 ± 0.8 2.1 ± 0.7 FVC (% predicted) 97 ± 12 108 ± 12 86 ± 13 71 ± 13 56 ± 14 FEV 1 /FVC ratio 0.79 ± 0.05 0.65 ± 0.04 0.58 ± 0.08 0.44 ± 0.09 0.32 ± 0.07 One or more acute respiratory disease episodes in the prior year to enrollment (%) 9 12 30 43 57
FEV 1 , forced expiratory volume in 1 second; FVC, forced vital capacity; GOLD, Global Initiative for Chronic Obstructive Lung Disease.
Data are presented as mean ± standard deviation or proportion (%).
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
TABLE 3
Effect of COPD Subjects’ Characteristics on FEV 1 at Baseline (mL) and on the Rate of Change in FEV 1 (mL/y) \*
Characteristic Baseline FEV 1 ( N = 4109) (mL) Rate of Change in FEV 1 ( N = 811) (mL/y) Estimate SE_P_ value Estimate † SE_P_ value Lung mass (per 100 g) 73.4 7.6 <0.0001 −4.7 1.7 0.006 Age (per 10 y) −142.3 11.9 <0.0001 2.7 2.6 0.30 Male gender 156.0 27.0 <0.0001 7.6 5.9 0.20 Height (per 5 cm) 115.2 7.6 <0.0001 3.2 1.6 0.051 Weight (per 5 kg) −22.0 2.9 <0.0001 −0.5 0.7 0.48 Current smoker −51.2 22.5 0.02 −12.5 4.8 0.009 Log %LAA-950 −272.1 10.7 <0.0001 −18.8 2.5 <0.0001 One or more acute respiratory disease episodes in the prior year to enrollment −310.5 19.5 <0.0001 −4.3 4.4 0.33 Baseline FEV 1 (mL) — — — −3.0 0.3 <0.0001
COPD, chronic obstructive pulmonary disease; FEV 1 , forced expiratory volume in 1 second; %LAA, percent low-attenuation area; SE, standard error
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Relationship Between LM and Change in FEV 1 in COPD Subjects
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Hogg J.C.: Pathophysiology of airflow limitation in chronic obstructive pulmonary disease. Lancet 2004; 364: pp. 709-721.
2. Nishimura M., Makita H., Nagai K., et. al.: Annual change in pulmonary function and clinical phenotype in chronic obstructive pulmonary disease. Am J Respir Crit Care Med 2012; 185: pp. 44-52.
3. Croxton T.L., Weinmann G.G., Senior R.M., et. al.: Clinical research in chronic obstructive pulmonary disease: needs and opportunities. Am J Respir Crit Care Med 2003; 167: pp. 1142-1149.
4. Han M.K., Agusti A., Calverley P.M., et. al.: Chronic obstructive pulmonary disease phenotypes: the future of COPD. Am J Respir Crit Care Med 2010; 182: pp. 598-604.
5. Coxson H.O., Leipsic J., Parraga G., et. al.: Using pulmonary imaging to move chronic obstructive pulmonary disease beyond FEV1. Am J Respir Crit Care Med 2014; 190: pp. 135-144.
6. Rosenkrantz A.B., Mendiratta-Lala M., Bartholmai B.J., et. al.: Clinical utility of quantitative imaging. Acad Radiol 2015; 22: pp. 33-49.
7. Hayhurst M.D., MacNee W., Flenley D.C., et. al.: Diagnosis of pulmonary emphysema by computerised tomography. Lancet 1984; 2: pp. 320-322.
8. Muller N.L., Staples C.A., Miller R.R., et. al.: “Density mask”. An objective method to quantitate emphysema using computed tomography. Chest 1988; 94: pp. 782-787.
9. Gevenois P.A., De Vuyst P., de Maertelaer V., et. al.: Comparison of computed density and microscopic morphometry in pulmonary emphysema. Am J Respir Crit Care Med 1996; 154: pp. 187-192.
10. Dirksen A., Dijkman J.H., Madsen F., et. al.: A randomized clinical trial of alpha(1)-antitrypsin augmentation therapy. Am J Respir Crit Care Med 1999; 160: pp. 1468-1472.
11. Parr D.G., Sevenoaks M., Deng C., et. al.: Detection of emphysema progression in alpha 1-antitrypsin deficiency using CT densitometry; methodological advances. Respir Res 2008; 9: pp. 21.
12. Vlahovic G., Russell M.L., Mercer R.R., et. al.: Cellular and connective tissue changes in alveolar septal walls in emphysema. Am J Respir Crit Care Med 1999; 160: pp. 2086-2092.
13. Guenard H., Diallo M.H., Laurent F., et. al.: Lung density and lung mass in emphysema. Chest 1992; 102: pp. 198-203.
14. Regan E.A., Hokanson J.E., Murphy J.R., et. al.: Genetic epidemiology of COPD (COPDGene) study design. COPD 2010; 7: pp. 32-43.
15. Standardization of Spirometry, 1994 Update. American Thoracic Society. Am J Respir Crit Care Med 1995; 152: pp. 1107-1136.
16. Crapo R.O., Morris A.H., Gardner R.M.: Reference spirometric values using techniques and equipment that meet ATS recommendations. Am Rev Respir Dis 1981; 123: pp. 659-664.
17. Rabe K.F., Hurd S., Anzueto A., et. al.: Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: GOLD executive summary. Am J Respir Crit Care Med 2007; 176: pp. 532-555.
18. Wan E.S., Hokanson J.E., Murphy J.R., et. al.: Clinical and radiographic predictors of GOLD-unclassified smokers in the COPDGene study. Am J Respir Crit Care Med 2011; 184: pp. 57-63.
19. Bowler R.P., Kim V., Regan E., et. al.: Prediction of acute respiratory disease in current and former smokers with and without COPD. Chest 2014; 146: pp. 941-950.
20. Diaz A.A., Han M.K., Come C.E., et. al.: Effect of emphysema on CT scan measures of airway dimensions in smokers. Chest 2013; 143: pp. 687-693.
21. Coxson H.O., Rogers R.M., Whittall K.P., et. al.: A quantification of the lung surface area in emphysema using computed tomography. Am J Respir Crit Care Med 1999; 159: pp. 851-856.
22. Henne E., Anderson J.C., Lowe N., et. al.: Comparison of human lung tissue mass measurements from ex vivo lungs and high resolution CT software analysis. BMC Pulm Med 2012; 12: pp. 18.
23. Vestbo J., Edwards L.D., Scanlon P.D., et. al.: Changes in forced expiratory volume in 1 second over time in COPD. N Engl J Med 2011; 365: pp. 1184-1192.
24. Bartel S.T., Bierhals A.J., Pilgram T.K., et. al.: Equating quantitative emphysema measurements on different CT image reconstructions. Med Phys 2011; 38: pp. 4894-4902.
25. Shaker S.B., Dirksen A., Lo P., et. al.: Factors influencing the decline in lung density in a Danish lung cancer screening cohort. Eur Respir J 2012; 40: pp. 1142-1148.
26. Karimi R., Tornling G., Forsslund H., et. al.: Lung density on high resolution computer tomography (HRCT) reflects degree of inflammation in smokers. Respir Res 2014; 15: pp. 23.
27. Shaker S.B., Stavngaard T., Laursen L.C., et. al.: Rapid fall in lung density following smoking cessation in COPD. COPD 2011; 8: pp. 2-7.
28. Leopold J.G., Gough J.: The centrilobular form of hypertrophic emphysema and its relation to chronic bronchitis. Thorax 1957; 12: pp. 219-235.
29. Hogg J.C., Chu F., Utokaparch S., et. al.: The nature of small-airway obstruction in chronic obstructive pulmonary disease. N Engl J Med 2004; 350: pp. 2645-2653.
30. Stockley R.A., Parr D.G., Piitulainen E., et. al.: Therapeutic efficacy of alpha-1 antitrypsin augmentation therapy on the loss of lung tissue: an integrated analysis of 2 randomised clinical trials using computed tomography densitometry. Respir Res 2010; 11: pp. 136.
31. Vestbo J., Agusti A., Wouters E.F., et. al.: Should we view chronic obstructive pulmonary disease differently after ECLIPSE? A clinical perspective from the study team. Am J Respir Crit Care Med 2014; 189: pp. 1022-1030.
32. Coxson H.O., Dirksen A., Edwards L.D., et. al.: The presence and progression of emphysema in COPD as determined by CT scanning and biomarker expression: a prospective analysis from the ECLIPSE study. Lancet Respir Med 2013; 1: pp. 129-136.