
Rationale and Objectives
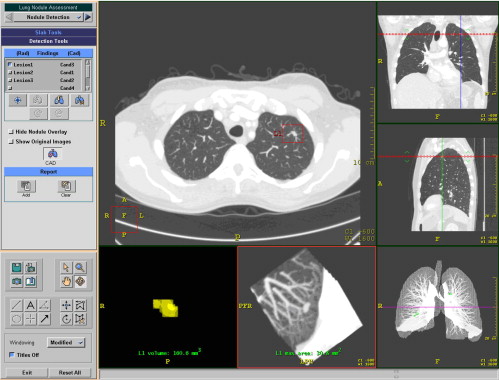
The purpose of this multicenter, multireader study was to evaluate the performance of computed tomography (CT) lung nodule computer-aided detection (CAD) software as a second reader.
Methods and Materials
The study involved 109 patients from four sites. The data were collected from a variety of multidetector CT scanners and had different scan parameters. Each chest CT scan was divided into four quadrants. A group of three expert thoracic radiologists identified nodules between 4 and 30 mm in maximum diameter within each quadrant. The standard of reference was established by a consensus read of these experienced radiologists. The cases were then interpreted by 10 other radiologist readers with varying degrees of experience, without and then with CAD software. These readers identified nodules and assigned an actionability rating to each quadrant before and after using CAD software. Receiver operating characteristic curves were used to measure the performance of the readers without and with CAD software.
Results
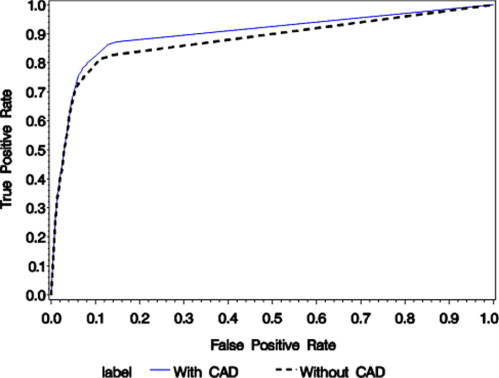
The average increase in area under the curve for the 10 readers with CAD software was 1.9% for a 95% confidence interval (0.8–8.0%). The area under the curve without CAD software was 86.7% and with CAD software was 88.7%. A nonsignificant correlation was observed between the improvement in sensitivity and experience of the radiologists. The readers also showed a greater improvement in patients with cancer as compared to those without cancer.
Conclusions
In this multicenter trial, CAD software was shown to be effective as a second reader by improving the sensitivity of the radiologists in detecting pulmonary nodules.
Detection and characterization of primary and metastatic lung cancer depends on successful identification of lung nodules on chest computed tomography (CT) scans ( ). Identification of indeterminate pulmonary nodules on chest multidetector CT (MDCT) scans is a common occurrence in routine radiology practice. It is clinically important to identify small nodules on a chest CT scan. A study by Wisnivesky et al showed that the smaller the size of the nodule more likely is the presence of Stage 1 lung cancer ( ). The location of the detected nodules is recorded for purposes of follow-up. In addition, change in size is valuable in characterization of a nodule. Malignant nodules usually have a faster doubling time compared with benign nodules. If a nodule remains unchanged for more than 2 years, it is conventionally designated as benign ( ).
Several studies have reported that radiologists often overlook nodules while interpreting chest CT scans ( ). This may be due to observational oversight or because of the large amount of data and increasing caseload produced by MDCT scanners. The newest generations of CT scanners allow isotropic scanning of the chest with high spatial resolution enabling identification of small pulmonary nodules. In this context, computer-aided detection (CAD) has been proposed by several researchers ( ) to facilitate accurate and efficient detection of lung nodules.
Get Radiology Tree app to read full this article<
Methods and materials
Patients
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
CT Scanning
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Radiologist Readers
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
CAD Software
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Table 1
Summary of Expert Results for Quadrants
Proportion of Expert Readers that Declared Quadrant to be Actionable Total 0/3 1/3 2/3 3/3 Number of quadrants 260 60 28 88 436
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 2
Actionable Quadrants Identified by Each Radiologist Reader Without and With CAD
Reader Number Level of Experience Actionable Quadrants Without CAD Actionable Quadrants With CAD Increase of Actionable Cancer Cases With CAD AURC Increase from CAD 95% Confidence Interval for AURC Increase Due to CAD 1 Moderate 52 71 12 4.2% (−1.1%, 13.0%) 2 High 79 79 0 0.0% (0.0%, 0.0%) 3 Minimal 79 82 2 0.5% (−0.5%, 0.0%) 4 Moderate 59 69 6 4.2% (1.3%, 18.3%) 5 High 71 73 2 0.2% (0.0%, 8.8%) 6 Moderate 77 79 1 0.5% (−1.5%, 7.2%) 7 High 78 81 3 0.2% (−2.3%, 0.0%) 8 Moderate 75 82 4 3.8% (−0.7%, 14.6%) 9 Minimal 63 72 7 5.2% (2.3%, 21.4%) 10 Moderate 80 83 2 0.7% (0.0%, 8.8%)
CAD, computer-aided detection; AURC, area under the receiver operating characteristic curve.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 3
Stand-Alone Sensitivity of CAD as a Function of the Slice Thickness
Nodule Group Number of Nodules Slice Thickness (mm) 0.9 1 1.25 2 2.5 3 Consensus nodules 91 80.8% 50.0% 66.7% 66.7% 33.3% 51.0%
CAD, computer-aided detection.
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Conclusion
Get Radiology Tree app to read full this article<
Acknowledgments
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Rubin G.D., Lyo J.K., Paik D.S., et. al.: Pulmonary nodule on multi-detector row CT scans: performance comparison of radiologists and computer-aided detection. Radiology 2005; 234: pp. 274-283.
2. Yankelwitz D., Wisnivesky J.P., Henschke C.I.: Stage of lung cancer in relation to its size: part 1. Chest 2005; 127: pp. 1132-1135.
3. Wisnivesky J.P., Yankelwitz D., Henschke C.I.: Stage of lung cancer in relation to its size: part 2. Chest 2005; 127: pp. 1136-1139.
4. Jennings G.S., Winer-Muram H.T., Tarver R.D., et. al.: Lung tumor growth: assessment with CT-comparison of diameter and cross-sectional area with volume measurements. Radiology 2004; 231: pp. 866-871.
5. Swensen S.J., Jett J.R., Sloan J.A., et. al.: Screening of lung cancer with low dose spiral computed tomography. Am J Respir Crit Care Med 2002; 20: pp. 911-920.
6. Peldschus K., Herzog P., Wood S., et. al.: Computer-aided diagnosis as a second reader: spectrum of findings in CT studies if chest interpreted as normal. Chest 2005; 123: pp. 1517-1523.
7. Beiden S.V., Wagner R.F., Campbell G.: Components-of-variance models and multiple-bootstrap experiments: an alternative method for random-effects, receiver operating characteristic analysis. Acad Radiol 2000; 7: pp. 341-349.
8. Armato S.G., Feng L., Giger M.L., et. al.: Lung cancer: performance of automated lung nodule detection applied to cancers missed in a CT screening program. Radiology 2002; 225: pp. 685-692.
9. Awai K., Murao K., Ozawa A., et. al.: Pulmonary nodules at chest CT: effect of computer-aided diagnosis on radiologists detection performance. Radiology 2004; 230: pp. 347-352.
10. Gurung J., Maataoui A., Khan M., et. al.: Automated detection of lung nodules in multidetector CT: influence of different reconstruction protocols on performance of a software prototype. Rofo 2006; 178: pp. 71-77.
11. Marten K., Grillhosl A., Seyfarth T., et. al.: Computer-assisted detection of pulmonary nodules: evaluation of diagnostic performance using an expert knowledge-based detection system with variable reconstruction slice thickness settings. Eur Radiol 2005; 15: pp. 203-212.
12. Kim J.S., Kim J.H., Cho J., et. al.: Automated detection of pulmonary nodules on CT images: effect of section thickness and reconstruction interval—initial results. Radiology 2005; 236: pp. 295-299.
13. Yuan R., Vos P.M., Cooperberg P.L.: Computer-aided detection in screening CT for pulmonary nodules. AJR Am J Roentegenol 2006; 186: pp. 1280-1287.
14. Armato S.G., McLennan G., McNitt-Gray M.F., et. al.: Lung image database consortium: developing a resource for the medical imaging research community. Radiology 2004; 232: pp. 739-748.
15. Marten K., Engelke C.: Computer-aided detection and automated CT volumetry of pulmonary nodules. Eur Radiol 2007; 17: pp. 888-901.