
Rationale and Objectives
To investigate the accuracy of dual-energy computed tomography in the depiction of perfusion defects in patients with acute pulmonary embolism (PE).
Materials and Methods
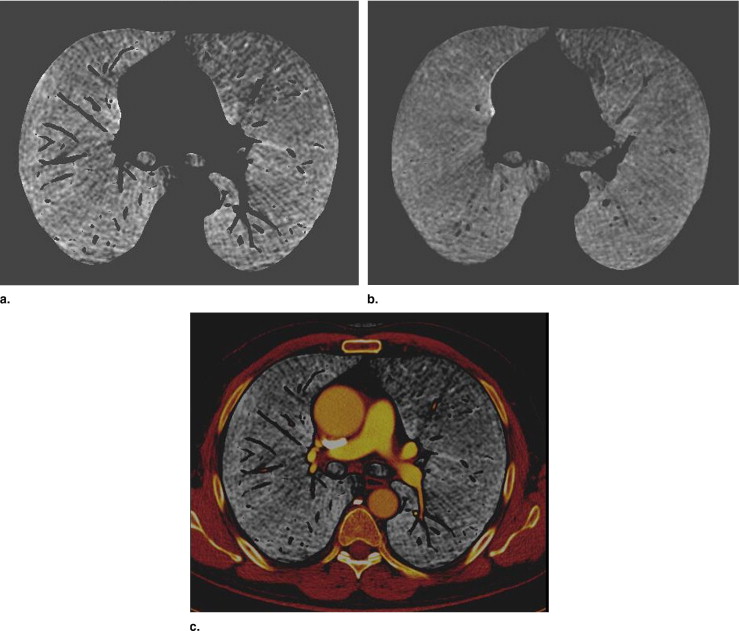
One hundred seventeen consecutive patients with clinical suspicion of acute PE underwent dual-energy multidetector computed tomographic (CT) angiography of the chest with a standard injection protocol. Two radiologists evaluated, by consensus, the presence of endoluminal clots on ( ) transverse “diagnostic” scans (contiguous 1-mm-thick averaged images from tubes A and B) and ( ) lung perfusion scans.
Results
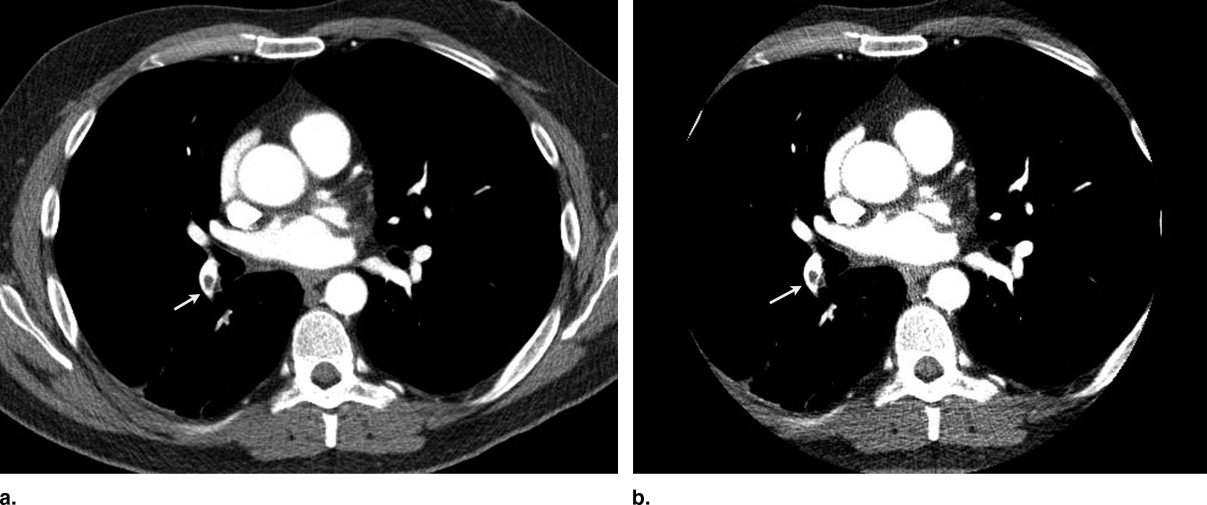
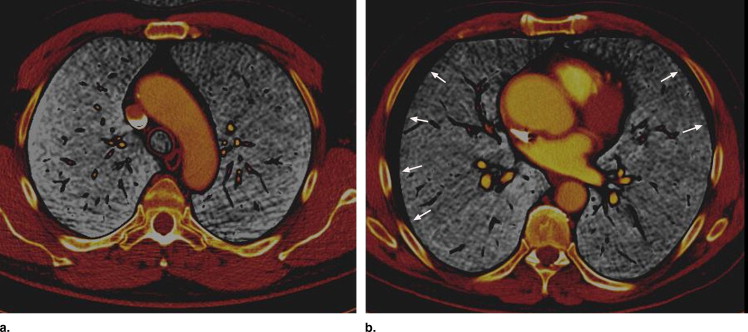
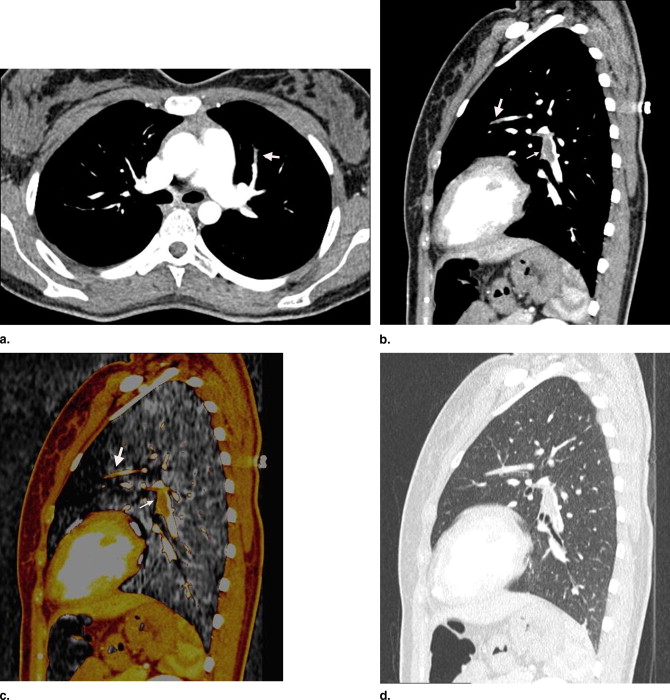
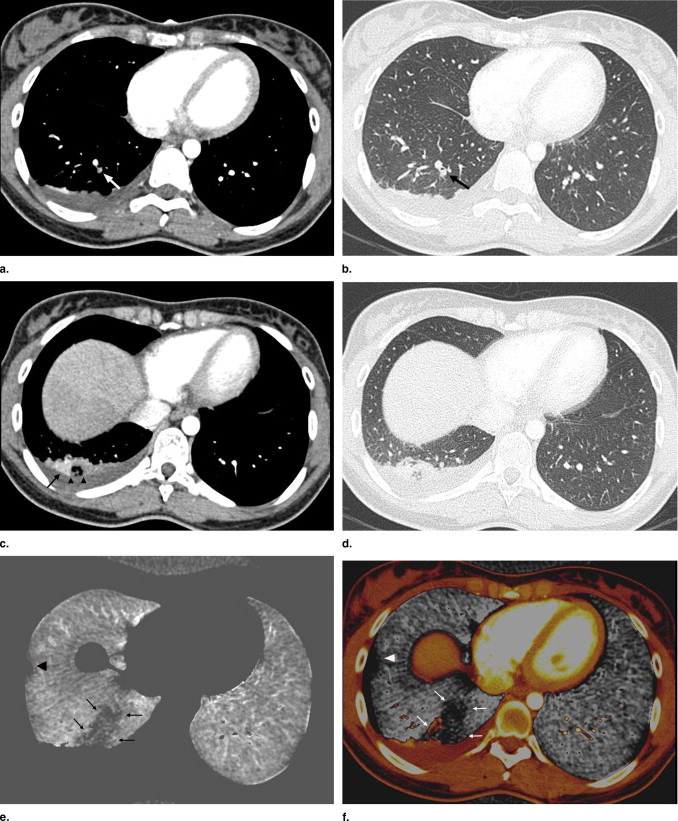
Seventeen patients showed CT features of acute PE, with the depiction of 75 clots within the lobar (n = 15), segmental (n = 43) and subsegmental (n = 17) pulmonary arteries. A total of 17 clots were identified as complete filling defects (ie, obstructive clots), located within segmental (12 of 17) and subsegmental (5 of 17) arteries. Fourteen of the 17 obstructive clots were seen with the concurrent presence of corresponding perfusion defects, whereas cardiac motion and/or contrast-induced artifacts precluded the confident recognition of perfusion abnormalities in the remaining two segments and one subsegment. Four subsegmental perfusion defects were depicted without the visualization of endoluminal thrombi within the corresponding arteries. Perfusion defects were identified beyond five nonobstructive clots.
Conclusion
Simultaneous information on the presence of endoluminal thrombus and lung perfusion impairment can be obtained with dual-energy computed tomography.
Since the introduction of multidetector-row computed tomography with high spatial and temporal resolution, computed tomographic (CT) angiography (CTA) has become the reference standard for diagnosing acute pulmonary embolism (PE), with sensitivity and specificity varying between 83% and 100% and 89 and 97%, respectively ( ). Although the depiction of endoluminal clots within central pulmonary arteries is an easy task, it may be more difficult to identify filling defects within small-sized pulmonary arteries. This potential limitation of CTA could be theoretically compensated for by the detection of ischemic lung zones beyond the level of obstructive clots, provided both morphologic and functional information can be derived from the same data set. Moreover, despite the availability of high-resolution images of pulmonary arteries, CTA does not allow the analysis of lung perfusion impairment after acute PE, which is especially valuable in patients with underlying respiratory disease.
On the basis of single-source computed tomography, two approaches have been investigated for the detection of perfusion abnormalities, one using color-coded maps of lung density in humans ( ) and the other a subtraction technique using pre- and postcontrast conventional CT images in experimental animal studies ( ). Although both approaches have demonstrated the detectability of perfusion defects on computed tomography, the feasibility of these approaches in clinical practice have substantial limitations pertaining to scanning times and levels of radiation exposure to patients. The recent availability of dual-source computed tomography and the subsequent possibility to scan patients with dual energy offers another alternative for lung functional imaging. Preliminary experiences have shown that this technique could be applied to the analysis of lung perfusion, with radiation doses below the legally required levels ( ). The purpose of this study was to investigate the detectability of perfusion defects with dual-energy computed tomography in the clinical context of acute PE.
Materials and methods
Population
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Scanning Protocol
Get Radiology Tree app to read full this article<
Reconstructed Scans
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
CT Parameters Analyzed
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Conditions of CT Interpretation
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results
Analysis of Diagnostic Scans
Overall Quality of Diagnostic Scans
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Detection of Endoluminal Clots
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Analysis of Perfusion Scans
Overall Quality of Perfusion Scans
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Analysis of Lung Perfusion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Radiation Dose for Dual-energy CTA
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Quanadli S.D., Hajjam M.E., Mesurolle B., et. al.: Pulmonary embolism detection: prospective evaluation of dual-section helical CT versus selective pulmonary arteriography in 157 patients. Radiology 2000; 217: pp. 447-455.
2. Winer-Muram H.T., Rydberg J., Johnson M.S., et. al.: Suspected acute pulmonary embolism: evaluation with multidetector row CT versus digital subtraction pulmonary arteriography. Radiology 2004; 233: pp. 806-815.
3. Stein P.D., Fowler S.E., Goodman L.R., et. al.: Multidetector computed tomography for acute pulmonary embolism [PIOPED II]. N Engl J Med 2006; 354: pp. 2317-2327.
4. Wildberger J.E., Niethammer M.U., Klotz E., et. al.: Multislice CT for visualization of pulmonary embolism using perfusion weighted color maps. Röfo 2001; 173: pp. 289-294.
5. Herzog P., Wildberger J.E., Niethammer M.U., et. al.: CT perfusion imaging of the lung in pulmonary embolism. Acad Radiol 2003; 10: pp. 1132-1146.
6. Coulden R.A., Brown S.J., Clements L., et. al.: Mosaic perfusion in pulmonary hypertension: how does multislice CT compare with perfusion scintigraphy. Radiology 2000; 217: pp. S384-S385.
7. Screaton N.J., Coxson H.O., Kalloger S.E., et. al.: Detection of lung perfusion abnormalities using computed tomography in a porcine model of pulmonary embolism. J Thorac Imaging 2003; 18: pp. 14-20.
8. Wildberger J.E., Klotz E., Ditt H., et. al.: Multislice computed tomography perfusion imaging for visualization of acute pulmonary embolism: animal experience. Eur Radiol 2005; 15: pp. 1378-1386.
9. Johnson T.R.C., Kraub B., Sedlmair M., et. al.: Material differentiation by dual energy CT: initial experience. Eur Radiol 2007; 17: pp. 1510-1517.
10. EC99.1999.European CommunityLuxembourg:pp. 69-78.
11. Sigal-Cinqualbre A.B., Hennequin R., Abada H.T., et. al.: Low-kilovoltage multidetector-row chest CT in adults: feasibility and effect on image quality and iodine dose. Radiology 2004; 231: pp. 169-174.
12. Schueller-Weidekamm C., Schaefer-Prokop C., Weber M., et. al.: CT angiography of pulmonary arteries to detect pulmonary embolism: improvement of vascular enhancement with low kilovoltage settings. Radiology 2006; 241: pp. 899-907.
13. Jackson C.L., Huber J.F.: Correlated applied anatomy of the bronchial tree and lungs with a system of nomenclature. Dis Chest 1943; 9: pp. 319-326.
14. Boyden E.A.: Segmental anatomy of the lungs.1955.McGraw-HillNew York
15. Brunot S., Corneloup O., Latrabe V., et. al.: Reproducibility of multidetector spiral computed tomography in detection of subsegmental acute pulmonary embolism. Eur Radiol 2005; 15: pp. 2057-2063.
16. Ritchie G., McGurk S., McCreath C., et. al.: Prospective evaluation of unsuspected pulmonary embolism on contrast enhanced multidetector CT (MDCT) scanning. Thorax 2007; 62: pp. 536-540.
17. Remy-Jardin M., Louvegny S., Remy J., et. al.: Acute central thromboembolic disease: posttherapeutic follow-up with spiral CT angiography. Radiology 1997; 203: pp. 173-180.
18. Goldhaber S.Z., Bounamoux H.: Thrombolytic therapy in pulmonary embolism. Semin Vasc Med 2001; 1: pp. 213-220.
19. Oser R.F., Zuckerman D.A., Guttierez F.R., Brinck J.A.: Anatomic distribution of pulmonary emboli at pulmonary angiography: implications for cross-sectional imaging. Radiology 1996; 199: pp. 31-35.
20. Diffin D.C., Leyendecker J.R., Johnson S.P., et. al.: Effect of anatomic distribution of pulmonary emboli on interobserver agreement in the interpretation of pulmonary angiography. AJR Am J Roentgenol 1998; 171: pp. 1085-1089.
21. de Monye W., van Strijen M.J., Huisman M.V., et. al.: Advances in New Technologies Evaluating the Localization of Pulmonary Embolism (ANTELOPE) Group. Radiology 2000; 215: pp. 184-188.
22. Remy-Jardin M., Remy J., Baghaie F., et. al.: Clinical value of thin collimation in the diagnostic workup of pulmonary embolism. AJR Am J Roentgenol 2000; 175: pp. 407-411.
23. Goodman L.R.: Small pulmonary emboli: what do we know?. Radiology 2005; 234: pp. 654-658.
24. Remy-Jardin M., Baghaie F., Bonnel F., et. al.: Thoracic helical CT: influence of subsecond scan time and thin collimation on evaluation of peripheral pulmonary arteries. Eur Radiol 2000; 10: pp. 1297-1303.
25. Ghaye B., Szapiro D., Mastora I., et. al.: Peripheral pulmonary arteries: how far in the lung can multidetector-row spiral CT allow analysis?. Radiology 2001; 219: pp. 629-636.
26. Schoepf U.J., Holzknecht N., Helmberger T.K., et. al.: Subsegmental pulmonary emboli: improved detection with thin-collimation multidetector-row spiral CT. Radiology 2002; 222: pp. 483-490.
27. Coche E., Pawlak S., Dechambre S., Maldague B.: Peripheral pulmonary arteries: identification at multislice spiral CT with 3D reconstruction. Eur Radiol 2003; 13: pp. 815-822.
28. Patel S., Kazerooni E.A., Cascade P.N.: Pulmonary embolism: optimization of small pulmonary artery visualization at multidetector-row CT. Radiology 2003; 227: pp. 455-460.
29. Jeong Y.J., Lee K.S., Yoon Y.C., et. al.: Evaluation of small pulmonary arteries by 16-slice multidetector computed tomography: optimum slab thickness in condensing transaxial images converted into maximum intensity projection. J Comput Assist Tomogr 2004; 28: pp. 195-203.
30. Amundsen T., Torheim G., Kvistad K.A., et. al.: Perfusion abnormalities in pulmonary embolism studied with perfusion MRI and ventilation-perfusion scintigraphy: an intra-modality and inter-modality agreement study. J Magn Reson Imaging 2002; 15: pp. 386-394.
31. Fink C., Bock M., Puderbach M., et. al.: Partially parallel three-dimensional magnetic resonance imaging for the assessment of lung perfusion-initial results. Invest Radiol 2003; 38: pp. 482-488.
32. Fink C., Ley S., Puderbach M., et. al.: 3D pulmonary perfusion MRI and MR angiography of pulmonary embolism in pigs after a single injection of a blood pool MR contrast agent. Eur Radiol 2004; 14: pp. 1291-1296.
33. Wolfkiel C.J., Rich S.: Analysis of regional pulmonary enhancement in dogs by ultrafast computed tomography. Invest Radiol 1992; 27: pp. 211-216.
34. Groell R., Peiche K.H., Uggowitzer M.M., et. al.: Computed tomography densitometry of the lung: a method to assess perfusion defects in acute pulmonary embolism. Eur Radiol 1999; 32: pp. 192-196.
35. Wildberger J.E., Mahnken A.H., Sinha A.M., et. al.: A differentiated approach to the diagnosis of pulmonary embolism and deep venous thrombosis using multislice CT. Fortschr Rontgenstr 2002; 174: pp. 301-307.
36. Christopher Study Investigators: Effectiveness of managing suspected pulmonary embolism using an algorithm combining clinical probability, d -dimer testing, and computed tomography. JAMA 2006; 295: pp. 172-179.
37. Perrier A., Roy P.M., Sanchez O., et. al.: Multidetector-row computed tomography in suspected pulmonary embolism. N Engl J Med 2005; 352: pp. 1760-1768.