
Rationale and Objectives
To investigate four-dimensional (4D) phase-contrast (PC) magnetic resonance (MR) in the evaluation of intracardiac shunts by simultaneous assessment of pulmonary (Q P ) and systemic (Q S ) flows in a pilot study and to compare results to through-plane two-dimensional (2D) PC MR.
Materials and Methods
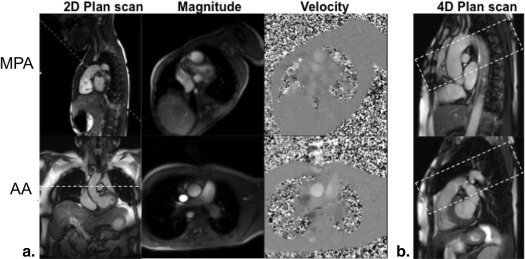
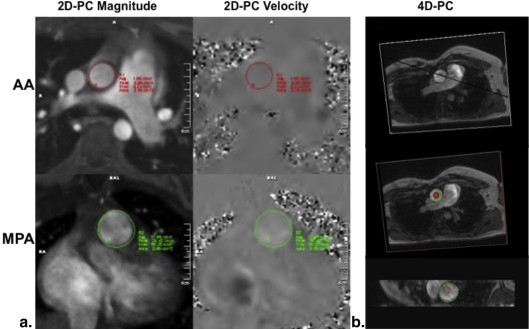
Institutional review board approval and written informed consent were obtained. Nineteen patients with suspected intracardiac shunts underwent cardiac MR at 1.5T. Assessments of Q P and Q S were performed using free-breathing retrospectively gated 2D PC gradient recalled echo (GRE; 1.6 × 1.6 × 5 mm 3 ) imaging with one-dimensional through-plane velocity encoding gradient (v enc = 150 cm/s) in consecutive measurements for the main pulmonary artery (MPA) and ascending aorta (AA), respectively. A prospectively triggered 4D PC GRE technique (2.4 × 1.8 × 3 mm 3 ) with three orthogonal v enc directions was also used with volume coverage of both MPA and AA.
Results
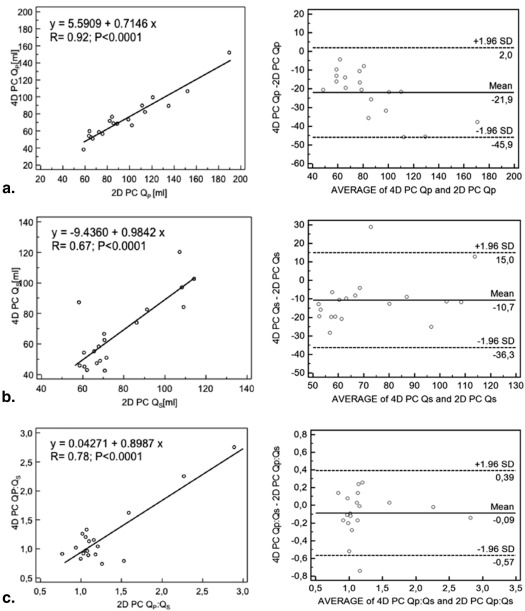
Q P and Q S assessed by 4D PC correlated with 2D PC acquisitions ( r = 0.92 and r = 0.67 respectively; P < .0001 for both) but demonstrated significant underestimation of individual flow volumes (−21.9 ± 12.2 mL; P < .0001 and −10.7 ± 13.1 mL; P = .0023, respectively). Calculated Q P :Q S ratios demonstrated high correlation ( r = 0.78; P < .0001) and no significant differences between 4D PC and 2D PC acquisitions (−0.09 ± 0.24, P = .14). Image acquisition times for 2D PC assessment of Q P and Q S were 2.98 ± 0.52 and 2.84 ± 0.50 minutes, respectively ( P = .038), whereas time to acquire 4D PC images was significantly longer, 18.75 ± 4.58 minutes ( P < .001).
Conclusions
Four-dimensional PC MR imaging allows for accurate assessment of Q P :Q S ratios in the evaluation of intracardiac shunts while absolute flow volumes demonstrate offsets. Further refinement of the technique with improvement in acquisition times may be required before widespread clinical implementation.
Atrial septal defect (ASD), ventricular septal defect (VSD), and patent ductus arteriosus (PDA) are among the most common congenital cardiac abnormalities . Shunt volumes and the ratio of flows in the pulmonary (Q P ) and systemic (Q S ) circulations are important measures in the evaluation of left-to-right shunts .
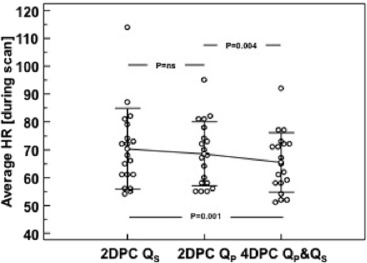
Multiple studies have demonstrated reliability of two-dimensional (2D) phase-contrast (PC) magnetic resonance imaging (MRI) in the assessment of Q P :Q S . Good agreement of 2D PC MRI with invasive oximetry, radionucleotide angiocardiography, and ventricular stroke volumes obtained by cine MRI have been previously reported . However, standard 2D PC magnetic resonance (MR) assessment of Q P :Q S performed with consecutive evaluation of the ascending aorta (AA) and main pulmonary artery (MPA) may be limited in accuracy by interval changes of hemodynamics such as heart rate (HR) that occur between separate PC measurements. Operator-related nonoptimized slice orientation may result in additional offsets for a single velocity encoding direction (along the slice selection direction-through-plane orientation) because of misalignment of slice encoding versus actual flow direction . As in other MR angiography techniques, special attention must be made during prescription of imaging planes .
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Materials and methods
Study Population
Get Radiology Tree app to read full this article<
Cardiac MRI
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Data Postprocessing
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 1
Phase-contrast Measurements ( n = 19)
Flow Correlation 2D PC 4D PC_P_ value_r_ value Q S (mL) 77.4 ± 19.1 66.7 ± 22.9 .001 0.67 Q P (mL) 96.4 ± 34.5 74.5 ± 25.7 .001 0.92 Q P :Q S 1.28 ± 0.51 1.19 ± 0.51 .001 0.78
Q P , pulmonary flow (main pulmonary artery); Q S , systemic flow (ascending aorta); 2D PC, two-dimensional phase-contrast acquisition; 4D PC, four-dimensional phase-contrast acquisition.
Data are mean ± standard deviation unless otherwise noted.
Correlation was assessed by Pearson correlation coefficient.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 2
Two-by-Two Table Comparing Shunt Identification by 4D PC to 2D PC Acquisition Using a Q P :Q S Cutoff of ≥1.5
Q P :Q S Cutoff ≥1.5 Total 2D PC + 2D PC − 4D PC + 3 (15.8) (TP) 0 (0.0) (FP) 3 (16) 4D PC − 1 (5.3) (FN) 15 (78.9) (TN) 16 (84) Total 4 (21) 15 (79) 19 (100)
FN, false negative; FP, false positive; TP, true positive; TN, true negative.
Data are represented as number of patients with percentages in parentheses.
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Acknowledgments
Get Radiology Tree app to read full this article<
References
1. Brickner M.E., Hillis L.D., Lange R.A.: Congenital heart disease in adults. First of two parts. N Engl J Med 2000; 342: pp. 256-263.
2. Warnes C.A., Williams R.G., Bashore T.M., et. al.: ACC/AHA 2008 guidelines for the management of adults with congenital heart disease: executive summary: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (writing committee to develop guidelines for the management of adults with congenital heart disease). Circulation 2008; 118: pp. 2395-2451.
3. Silversides C.K., Marelli A., Beauchesne L., et. al.: Canadian cardiovascular society 2009 consensus conference on the management of adults with congenital heart disease: executive summary. Can J Cardiol 2010; 26: pp. 143-150.
4. Debl K., Djavidani B., Buchner S., et. al.: Quantification of left-to-right shunting in adult congenital heart disease: Phase-contrast cine MRI compared with invasive oximetry. Br J Radiol 2009; 82: pp. 386-391.
5. Beerbaum P., Korperich H., Gieseke J., et. al.: Rapid left-to-right shunt quantification in children by phase-contrast magnetic resonance imaging combined with sensitivity encoding (SENSE). Circulation 2003; 108: pp. 1355-1361.
6. Arheden H., Holmqvist C., Thilen U., et. al.: Left-to-right cardiac shunts: Comparison of measurements obtained with MR velocity mapping and with radionuclide angiography. Radiology 1999; 211: pp. 453-458.
7. Petersen S.E., Voigtlander T., Kreitner K.F., et. al.: Quantification of shunt volumes in congenital heart diseases using a breath-hold MR phase contrast technique—comparison with oximetry. Int J Cadiovasc Img 2002; 18: pp. 53-60.
8. Gatehouse P.D., Keegan J., Crowe L.A., et. al.: Applications of phase-contrast flow and velocity imaging in cardiovascular MRI. Eur Radiol 2005; 15: pp. 2172-2184.
9. Mohiaddin R.H., Underwood R., Romeira L., et. al.: Comparison between cine magnetic resonance velocity mapping and first-pass radionuclide angiocardiography for quantitating intracardiac shunts. Am J Cardiol 1995; 75: pp. 529-532.
10. Brenner L.D., Caputo G.R., Mostbeck G., et. al.: Quantification of left to right atrial shunts with velocity-encoded cine nuclear magnetic resonance imaging. J Am Coll Cardiol 1992; 20: pp. 1246-1250.
11. Lotz J., Meier C., Leppert A., et. al.: Cardiovascular flow measurement with phase-contrast MR imaging: basic facts and implementation. Radiographics 2002; 22: pp. 651-671.
12. Shariat M., Schantz D., Yoo S., et. al.: Pulmonary artery pulsatility and effect on vessel diameter assessment in magnetic resonance imaging. Eur J Radiol 2014; 83: pp. 378-383.
13. Markl M., Kilner P.J., Ebbers T.: Comprehensive 4D velocity mapping of the heart and great vessels by cardiovascular magnetic resonance. J Cardiovasc Magn Reson 2011; 13: pp. 7.
14. Stalder A.F., Russe M.F., Frydrychowicz A., et. al.: Quantitative 2D and 3D phase contrast MRI: Optimized analysis of blood flow and vessel wall parameters. Magn Reson Med 2008; 60: pp. 1218-1231.
15. Francois C.J., Srinivasan S., Schiebler M.L., et. al.: 4D cardiovascular magnetic resonance velocity mapping of alterations of right heart flow patterns and main pulmonary artery hemodynamics in tetralogy of Fallot. J Cardiovasc Magn Reson 2012; 14: pp. 16.
16. Beerbaum P., Korperich H., Barth P., et. al.: Noninvasive quantification of left-to-right shunt in pediatric patients: phase-contrast cine magnetic resonance imaging compared with invasive oximetry. Circulation 2001; 103: pp. 2476-2482.
17. Wigstrom L., Sjoqvist L., Wranne B.: Temporally resolved 3D phase-contrast imaging. Magn Reson Med 1996; 36: pp. 800-803.
18. Markl M., Draney M.T., Hope M.D., et. al.: Time-resolved 3-dimensional velocity mapping in the thoracic aorta: Visualization of 3-directional blood flow patterns in healthy volunteers and patients. J Comput Assist Tomogr 2004; 28: pp. 459-468.
19. Markl M., Chan F.P., Alley M.T., et. al.: Time-resolved three-dimensional phase-contrast MRI. J Magn Reson Imaging 2003; 17: pp. 499-506.
20. Carlsson M., Toger J., Kanski M., et. al.: Quantification and visualization of cardiovascular 4D velocity mapping accelerated with parallel imaging or k-t BLAST: Head to head comparison and validation at 1.5 T and 3 T. J Cardiovasc Magn Reson 2011; 13: pp. 55.
21. Hsiao A., Lustig M., Alley M.T., et. al.: Evaluation of valvular insufficiency and shunts with parallel-imaging compressed-sensing 4D phase-contrast MR imaging with stereoscopic 3D velocity-fusion volume-rendered visualization. Radiol 2012; 265: pp. 87-95.
22. Westenberg J.J., Roes S.D., Ajmone Marsan N., et. al.: Mitral valve and tricuspid valve blood flow: accurate quantification with 3D velocity-encoded MR imaging with retrospective valve tracking. Radiol 2008; 249: pp. 792-800.
23. Chernobelsky A., Shubayev O., Comeau C.R., et. al.: Baseline correction of phase contrast images improves quantification of blood flow in the great vessels. J Cardiovasc Magn Reson 2007; 9: pp. 681-685.
24. Miller T.A., Landes A.B., Moran A.M.: Improved accuracy in flow mapping of congenital heart disease using stationary phantom technique. J Cardiovasc Magn Reson 2009; 11: pp. 52.
25. Ley S., Fink C., Puderbach M., et. al.: MRI measurement of the hemodynamics of the pulmonary and systemic arterial circulation: influence of breathing maneuvers. Am J Roentgenol 2006; 187: pp. 439-444.
26. Ley S., Ley-Zaporozhan J., Kreitner K., et. al.: MR flow measurements for assessment of the pulmonary, systemic and bronchosystemic circulation: impact of different ECG gating methods and breathing schema. Eur J Radiol 2007; 61: pp. 124-129.
27. Marshall I.: Feasibility of k-t BLAST technique for measuring “seven-dimensional” fluid flow. J Magn Reson Imaging 2006; 23: pp. 189-196.
28. Johnson K.M., Lum D.P., Turski P.A., et. al.: Improved 3D phase contrast MRI with off-resonance corrected dual echo VIPR. Magn Reson Med 2008; 60: pp. 1329-1336.
29. Uribe S., Beerbaum P., Sorensen T.S., et. al.: Four-dimensional (4D) flow of the whole heart and great vessels using real-time respiratory self-gating. Magn Reson Med 2009; 62: pp. 984-992.
30. Roes S.D., Hammer S., van der Geest R.J., et. al.: Flow assessment through four heart valves simultaneously using 3-dimensional 3-directional velocity-encoded magnetic resonance imaging with retrospective valve tracking in healthy volunteers and patients with valvular regurgitation. Invest Radiol 2009; 44: pp. 669-675.