
Rationale and Objectives
To determine if intraprostatic injection of gadofosveset trisodium mixed with human serum albumin (HSA) can identify sentinel lymph nodes (LNs) draining the prostate on magnetic resonance imaging (MRI) in a canine model.
Materials and Methods
Three male canines weighing between 25.7 and 41.3 kg were anesthetized, placed in a 3-T MRI, and a needle was placed transrectally into one side of the prostate using a commercially available intrarectal needle guide. Gadofosveset trisodium premixed with 10% HSA was then administered at doses ranging from 0.1 to 2.5 mL. T1W MRI was performed immediately after injection, and two readers evaluated images for visualization of LNs draining the prostate.
Results
Intraprostatic injection of 0.2 mL gadofosveset trisodium premixed with HSA identified the draining periprostatic LNs in all cases. Delayed images demonstrated upper echelon nodes in the pelvis and the abdomen. Higher volume injections resulted in excessive periprostatic extravasation, whereas lower volume injections resulted in suboptimal visualization of LNs.
Conclusions
We demonstrate that gadofosveset trisodium (premixed with 10% HSA) injected intraprostatically at 0.2 mL visualized LNs draining the prostate. This approach can be readily adapted for clinical applications such as sentinel LN imaging in prostate cancer patients before surgery.
Identification of lymph node metastasis is important for the accurate staging of prostate cancer (PCa). Current anatomic and functional imaging techniques have limited accuracy in the detection of metastatic lymph nodes (LNs) . Therefore, surgical pelvic LN dissection (PLND) remains the gold standard for nodal staging . The most common surgical approach to PLND includes resection of nodes in the obturator fossa; however, this technique fails to detect almost 30% of metastatic LNs . For this reason, extended PLND (EPLND), including additional pelvic wall nodes and iliac LN chains, is currently the preferred method in higher risk patients . Although decreasing the false-negative rate for PCa, EPLND results in more complications such as lymphoceles, thromboembolic events, ureteral injury, and neurovascular injury due to the invasiveness of the surgery , and therefore, a more targeted approach to LN resection is desirable.
A variety of imaging approaches have been used to identify malignant nodes in the pelvis. Computed tomography and magnetic resonance (MR) imaging (MRI) use size criteria to judge whether a node is malignant. Unfortunately, both methods experience a low sensitivity and specificity around 0.39–0.42 and 0.82, respectively . Recently, functional MRI, specifically diffusion-weighted MRI, has been used to detect normal-sized metastatic nodes in patients with prostate and bladder cancer diagnosed as N0 with conventional cross-sectional imaging techniques . However, these results require further validation as the specificity may not be sufficient for clinical purposes. MRI performed 24 hours after intravenous injection of an ultrasmall superparamagnetic iron oxide agent has been reported to identify metastatic nodes by the absence of uptake of iron. However, this method is not yet widely available as the ideal agent, ferumoxtran, is not currently commercially available . Positron emission tomography with fluorodeoxyglucose has a low sensitivity in PCa but good specificity for nodal metastases .
Get Radiology Tree app to read full this article<
Materials and methods
Contrast Agent
Get Radiology Tree app to read full this article<
Study Design
Get Radiology Tree app to read full this article<
In Vivo Imaging
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 1
Pulse Sequence Parameters Used for SLN MRI After Gadofosveset Trisodium Injection
TR/TE (ms) Matrix Field of View (mm) Slice Thickness (mm) Flip Angle Voxel Size (mm × mm × mm) Fat Suppression Acquisition Time (s) 6.1/2.9 508 × 200 306 × 200 × 180 1.2 25 0.6 × 0.6 × 0.6 SPIR 218
MRI, magnetic resonance imaging; SLN, sentinel lymph node; TR, repetition time; TE, echo time; SPIR, spectral presaturation with inversion recovery.
Get Radiology Tree app to read full this article<
Image Analysis
Get Radiology Tree app to read full this article<
Results
Intraprostatic Injection of 2.0–2.5 mL Gadofosveset Trisodium Premixed with 10% Human Serum Albumin
Get Radiology Tree app to read full this article<
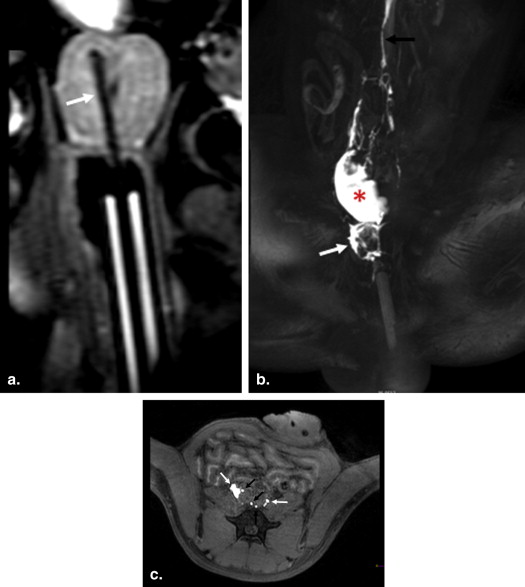
Get Radiology Tree app to read full this article<
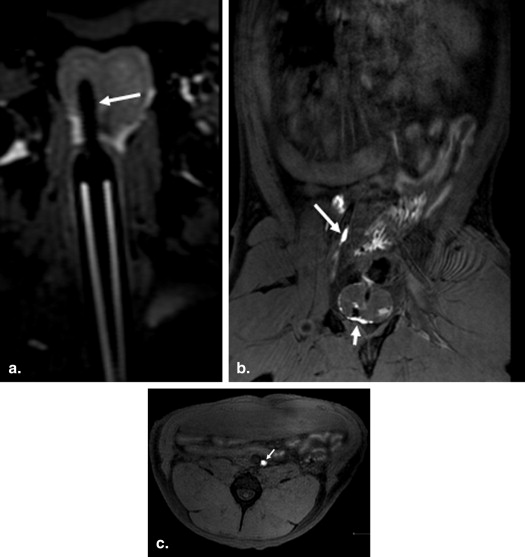
Intraprostatic Injection of 0.5-mL Gadofosveset Trisodium Premixed with 10% Human Serum Albumin
Get Radiology Tree app to read full this article<
Intraprostatic Injection of 0.2-mL Gadofosveset Trisodium Premixed with 10% Human Serum Albumin
Get Radiology Tree app to read full this article<
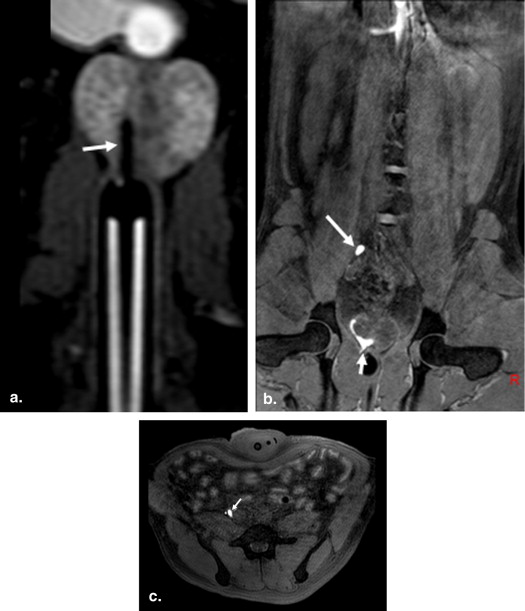
Get Radiology Tree app to read full this article<
Intraprostatic Injection of 0.1-mL Gadofosveset Trisodium Premixed with 10% Human Serum Albumin
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Table 2
Summary of Experimental Results in This Study
Dog Number Dog Weight (kg) Prostate Size (mL) Injected Dose (mL/Lobe) Injection Site Visualized Lymph Node Chains Visibility Window (min) Periprostatic Leak 1 41.3 25 2.5 Left R common iliac, retroperitoneal 0–30 Large 2 28 21 2 Right R common iliac, retroperitoneum 0–30 Large 3 25.7 27 0.5 Left L internal iliac, bilateral common iliac 0–21 Moderate 3 25.7 27 0.5 Right Bilateral common iliac 0–30 Moderate 1 38.6 25 0.2 Right R common iliac, retroperitoneal 0–30 Small 2 29.1 21 0.2 Right R common iliac, retroperitoneum 0–30 Small 3 26.5 27 0.2 Left L internal iliac, L common iliac 7–30 Small 1 39 25 0.1 Right R common iliac, retroperitoneum 0–21 Minimal 1 39 25 0.1 Left L common iliac 0–14 Minimal 3 26.5 27 0.1 Right R common iliac 0–7 None
L, left; R, right.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Acknowledgments
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Tiguert R., Gheiler E.L., Tefilli M.V., et. al.: Lymph node size does not correlate with the presence of prostate cancer metastasis. Urology 1999; 53: pp. 367-371.
2. Oyen R.H., Van Poppel H.P., Ameye F.E., et. al.: Lymph node staging of localized prostatic carcinoma with CT and CT-guided fine-needle aspiration biopsy: prospective study of 285 patients. Radiology 1994; 190: pp. 315-322.
3. Heidenreich A., Aus G., Bolla M., et. al.: EAU guidelines on prostate cancer. Eur Urol 2008; 53: pp. 68-80.
4. Bader P., Burkhard F.C., Markwalder R., et. al.: Is a limited lymph node dissection an adequate staging procedure for prostate cancer?. J Urol 2002; 168: pp. 514-518.
5. Briganti A., Blute M.L., Eastham J.H., et. al.: Pelvic lymph node dissection in prostate cancer. Eur Urol 2009; 55: pp. 1251-1265.
6. Clark T., Parekh D.J., Cookson M.S., et. al.: Randomized prospective evaluation of extended versus limited lymph node dissection in patients with clinically localized prostate cancer. J Urol 2003; 169: pp. 145-147. discussion 147–148
7. Hövels A., Heesakkers R., Adang E., et. al.: The diagnostic accuracy of CT and MRI in the staging of pelvic lymph nodes in patients with prostate cancer: a meta-analysis. Clin Radiol 2008; 63: pp. 387-395.
8. Thoeny H.C., Froehlich J.M., Triantafyllou M., et. al.: Metastases in normal-sized pelvic lymph nodes: detection with diffusion-weighted MR imaging. Radiology 2014; 273: pp. 125-135.
9. Harisinghani M.G., Barentsz J., Hahn P.F., et. al.: Noninvasive detection of clinically occult lymph-node metastases in prostate cancer. N Engl J Med 2003; 348: pp. 2491-2499.
10. Schöder H., Herrmann K., Gönen M., et. al.: 2-[18F]fluoro-2-deoxyglucose positron emission tomography for the detection of disease in patients with prostate-specific antigen relapse after radical prostatectomy. Clin Cancer Res 2005; 11: pp. 4761-4769.
11. Jeschke S., Beri A., Grüll M., et. al.: Laparoscopic radioisotope-guided sentinel lymph node dissection in staging of prostate cancer. Eur Urol 2008; 53: pp. 126-132.
12. Beri A., Janetschek G.: Technology insight: radioguided sentinel lymph node dissection in the staging of prostate cancer. Nat Clin Pract Urol 2006; 3: pp. 602-610.
13. Ganswindt U., Schilling D., Müller A.C., et. al.: Distribution of prostate sentinel nodes: a SPECT-derived anatomic atlas. Int J Radiat Oncol Biol Phys 2011; 79: pp. 1364-1372.
14. Jeschke S., Nambirajan T., Leeb K., et. al.: Detection of early lymph node metastases in prostate cancer by laparoscopic radioisotope guided sentinel lymph node dissection. J Urol 2005; 173: pp. 1943-1946.
15. Lauffer R.B., Parmelee D.J., Ouellet H.S., et. al.: MS-325: a small-molecule vascular imaging agent for magnetic resonance imaging. Acad Radiol 1996; 3: pp. S356-S358.
16. Nakajima T., Turkbey B., Sano K., et. al.: MR lymphangiography with intradermal gadofosveset and human serum albumin in mice and primates. J Magn Reson Imaging 2014; 40: pp. 691-697.
17. Turkbey B., Kobayashi H., Hoyt R.F., et. al.: Magnetic resonance lymphography of the thoracic duct after interstitial injection of gadofosveset trisodium: a pilot dosing study in a porcine model. Lymphat Res Biol 2014; 12: pp. 32-36.
18. Hambrock T., Fütterer J.J., Huisman H.J., et. al.: Thirty-two-channel coil 3T magnetic resonance-guided biopsies of prostate tumor suspicious regions identified on multimodality 3T magnetic resonance imaging: technique and feasibility. Invest Radiol 2008; 43: pp. 686-694.
19. Kiselev M.A., Gryzunov Iu.A., Dobretsov G.E., et. al.: Size of a human serum albumin molecule in solution. Biofizika 2001; 46: pp. 423-427.
20. Ikomi F., Hanna G.K., Schmid-Schönbein G.W.: Mechanism of colloidal particle uptake into the lymphatic system: basic study with percutaneous lymphography. Radiology 1995; 196: pp. 107-113.
21. Lu Q., Bui D., Liu N.F., et. al.: Magnetic resonance lymphography at 3T: a promising noninvasive approach to characterise inguinal lymphatic vessel leakage. Eur J Vasc Endovasc Surg 2012; 43: pp. 106-111.
22. Holl G., Dorn R., Wengenmair H., et. al.: Validation of sentinel lymph node dissection in prostate cancer: experience in more than 2,000 patients. Eur J Nucl Med Mol Imaging 2009; 36: pp. 1377-1382.
23. Rousseau C., Rousseau T., Bridji B., et. al.: Laparoscopic sentinel lymph node (SLN) versus extensive pelvic dissection for clinically localized prostate carcinoma. Eur J Nucl Med Mol Imaging 2012; 39: pp. 291-299.
24. van der Poel H.G., Buckle T., Brouwer O.R., et. al.: Intraoperative laparoscopic fluorescence guidance to the sentinel lymph node in prostate cancer patients: clinical proof of concept of an integrated functional imaging approach using a multimodal tracer. Eur Urol 2011; 60: pp. 826-833.