
Rationale and Objectives
The aim of this study was to determine if patients who underwent partial-breast irradiation followed by segmental mastectomies had fewer mammographic changes on the first post-treatment mammogram than those who underwent segmental mastectomies followed by whole-breast irradiation.
Materials and Methods
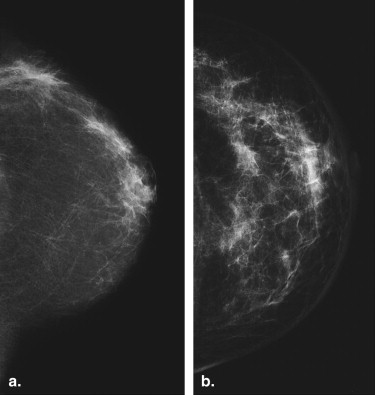
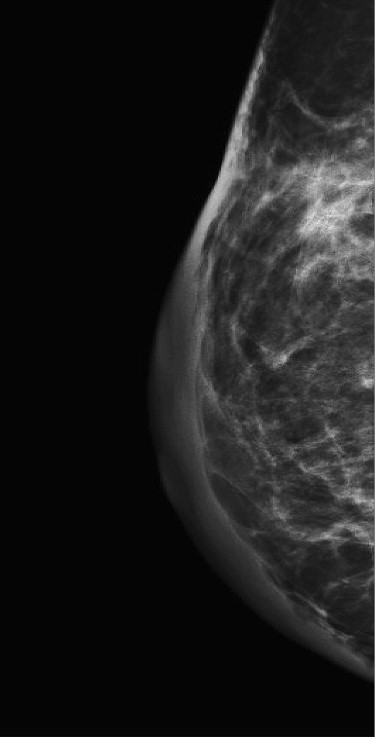
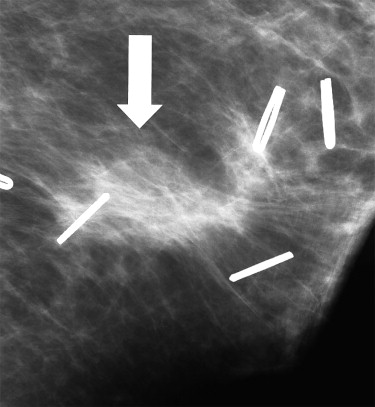
Subjects enrolled in a study of partial-breast irradiation therapy after segmental mastectomy (intraoperative radiation therapy) plus a random sample of patients who underwent segmental mastectomies followed by conventional whole-breast radiation therapy were identified through the institution’s breast cancer database from March 2003 through February 2006. A radiologist specializing in breast imaging reviewed and recorded each patient’s pretreatment mammogram for breast density and tumor location and the first post-treatment mammogram, obtained within the first year of treatment, for three common types of mammographic change seen after breast surgery and radiation treatment (breast edema, skin thickening, and surgical scarring), which when severe make it difficult to use mammography for continuing follow-up of the conserved breast. The extent of mammographic change was noted by the radiologist as minimal, moderate, or marked. The data were entered into a database, and statistical analysis was conducted using logistic regression models and χ 2 tests. The effect of breast density on mammographic change was also assessed.
Results
The severity of edema was lower with decreasing breast density ( P < .006). There was no apparent effect of breast density on the severity of skin thickening. The extent of surgical scarring decreased as breast density increased ( P < .026). Analysis of the data from the cumulative logistic regression models demonstrated that even after controlling for breast density, patients who underwent whole-breast radiation therapy had significantly more edema ( P = .003), skin thickening ( P = .003), and surgical scarring than those who underwent intraoperative radiation therapy ( P < .001).
Conclusion
Patients have a higher probability of having fewer post-treatment mammographic changes after partial-breast irradiation followed by segmental mastectomy than after breast conservation surgery followed by whole-breast irradiation.
Segmental mastectomy followed by whole-breast radiation therapy (WBRT) has been validated in several clinical trials and is now the standard of care for patients undergoing breast conservation therapy for breast cancer . However, barriers to appropriate long courses of radiotherapy may be due to patients’ receiving inadequate breast conservation therapy . Consequently, accelerated partial-breast irradiation as intraoperative radiation therapy (IORT) is a novel technique, as seen in Figure 1 , that has been proposed to reduce the time a patient spends in radiation therapy . Because the majority of recurrent breast cancers occur at the lumpectomy site, whereas recurrences in other quadrants of the breast occur with similar frequency in irradiated and nonirradiated patients, this suggests that the success of radiotherapy is related to the eradication of residual disease in the lumpectomy bed itself . Nevertheless, breast cancer recurrence may be equally well controlled by IORT because it delivers a larger dose per fraction over a smaller volume without increasing normal-tissue toxicity .
 Open full size image
Open full size image
Figure 1
Intraoperative radiation therapy. Radiation cone in place over lumpectomy site with skin retracted.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Materials and methods
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 1
Breast Density and Cancer Distribution in the IORT and WBRT Patients
Finding IORT WBRT Breast density Fatty 5 (15.6%) 4 (12.5%) Scattered fibroglandular densities 17 (53.1%) 17 (53.1%) Heterogeneously dense 6 (18.8%) 8 (25%) Extremely dense 4 (12.5%) 3 (9.4%) Cancer total 32 32 Right breast 10 (31.3%) 19 (59.3%) Left breast 22 (68.7%) 13 (40.7%) Cancer location Upper outer quadrant 14 (43.8%) 20 (62.5%) Upper inner quadrant 4 (12.5%) 5 (15.6%) Lower inner quadrant 5 (15.6%) 4 (12.5%) Lower outer quadrant 6 (18.8%) 0 (0.0%) Subareolar location 3 (9.3%) 3 (9.3%)
IORT, intraoperative radiation therapy; WBRT, whole-breast radiation therapy.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
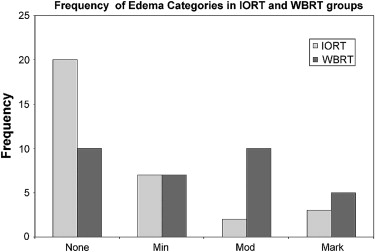
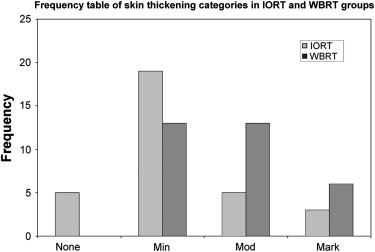
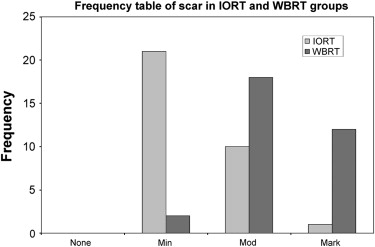
Table 2
χ 2 P Values for Comparison of Performance Between Intraoperative Radiation Therapy and Whole-Breast Radiation Therapy
Mammographic Finding_P_ Value Edema .028 Skin thickening .006 Scarring <.001
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Conclusion
Get Radiology Tree app to read full this article<
References
1. Veronesi U., Zucalli R., Luini A.: Local control and survival in early breast cancer: the Milan Trial. Int J Radiat Oncol Biol Phys 1986; 12: pp. 717-720.
2. Fisher B., Redmont C., Poisson R., et. al.: Eight year result of a randomized clinical trial comparing total mastectomy and lumpectomy with or without irradiation in the treatment of breast cancer. N Engl J Med 1989; 320: pp. 822-828.
3. Sarrazin D., Le M.G., Arriagada R., et. al.: Ten-year results of a randomized trial comparing a conservative treatment to mastectomy in early breast cancer. Radiother Oncol 1989; 14: pp. 177-184.
4. Fisher B., Anderson S., Redmond C.K., et. al.: Reanalysis and results after 12 years of follow-up in a randomized clinical trial comparing total mastectomy with lumpectomy with or without irradiation in the treatment of breast cancer. N Engl J Med 1995; 333: pp. 1456-1461.
5. Veronesi U., Luini A., Del Vecchio M., et. al.: Radiotherapy after breast-preserving surgery in women with localized cancer of the breast. N Engl J Med 1993; 328: pp. 1578-1591.
6. Ballard-Barbash R., Potosky A.L., Harlan L.C., et. al.: Factors associated with surgical and radiation therapy for early stage breast cancer in older women. J Natl Cancer Inst 1996; 88: pp. 716-726.
7. Morrow M., White J., Moughan J., et. al.: Factors predicting the use of breast-conserving therapy in stage I and II breast carcinomas. J Clin Oncol 2001; 19: pp. 2254-2262.
8. Ollila D.W., Klauber-DeMore N., Tesche L.J., Kuzmiak C.M., Pavic D., Goyal L.V.: Feasibility of breast preserving therapy with single fraction in situ radiotherapy delivered intraoperatively. Ann Surg Oncol 2005; 14: pp. 660-669.
9. Liljegren G., Holmberg L., Bergh J., et. al.: 10-year results after sector resection with or without postoperative radiotherapy for stage I breast cancer: a randomized trial. J Clin Oncol 1999; 17: pp. 2326-2333.
10. Veronesi U., Marubini E., Mariani L., et. al.: Radiotherapy after breast-conserving surgery in small breast carcinoma: long-term results of a randomized trial. Ann Oncol 2001; 12: pp. 997-1003.
11. Clark R.M., Wilkinson R.H., Miceli P.N., et. al.: Breast cancer. Experience with conservation therapy. Am J Clin Oncol 1987; 10: pp. 462-468.
12. Vicini F., Arthur D., Polgar C., et. al.: Defining the efficacy of accelerated partial breast irradiation: the importance of proper patient selection, optimal quality assurance and common sense. Int J Radiat Oncol Biol Phys 2003; 57: pp. 1210-1213.
13. Smith T.E., Lee D., Turner B.C., et. al.: True recurrence vs. new primary ipsilateral breast tumor relapse: an analysis of clinical and pathologic differences and their implications in natural history, prognoses, therapeutic management. Int J Tradiat Oncol Biol Phys 2000; 48: pp. 1281-1289.
14. Krishnamurthy R., Whitman G.J., Stelling C.B., et. al.: Mammographic findings after breast conservation therapy. Radiographics 1999; 19: pp. S53-S62.
15. Cardenosa C.: Breast imaging.2004.Lippincott, Williams & WilkinsPhiladelphia
16. Stomper P.C., Recht A., Berenberg A.L., Jochelson M.S., Harris J.R.: Mammographic detection of recurrent cancer in the irradiated breast. AJR Am J Roentgenol 1987; 148: pp. 39-43.
17. Nelder J., Wedderburn R.: Generalized linear models. J Royal Stat Soc Ser A (Gen) 1972; 135: pp. 370-384.
18. Greenwood P.E., Nikulin M.S.: A guide to chi-squared testing.1996.John WileyNew York
19. American College of Radiology : Breast Imaging Reporting and Data System.3rd ed1998.American College of RadiologyReston, VA
20. Della Sala S.W., Pellegrini M., Bernardi D., et. al.: Mammographic and ultrasonographic comparison between intraoperative radiotherapy (IORT) and conventional external radiotherapy in limited-stage breast cancer conservatively treated. Eur Radiol 2006; 59: pp. 222-230.
21. Wasser K., Schoeber C., Kraus-Tiefenbacher U., et. al.: Early mammographic and sonographic findings after intraoperative radiotherapy (IORT) as a boost in patients with breast cancer. Eur Radiol 2007; 17: pp. 1865-1874.