
Rationale and Objectives
The aim of the present study was to examine the usefulness and record the complications of preoperative lipiodol marking using computed tomographic (CT) fluoroscopy for the intraoperative localization of 107 pulmonary nodules.
Methods
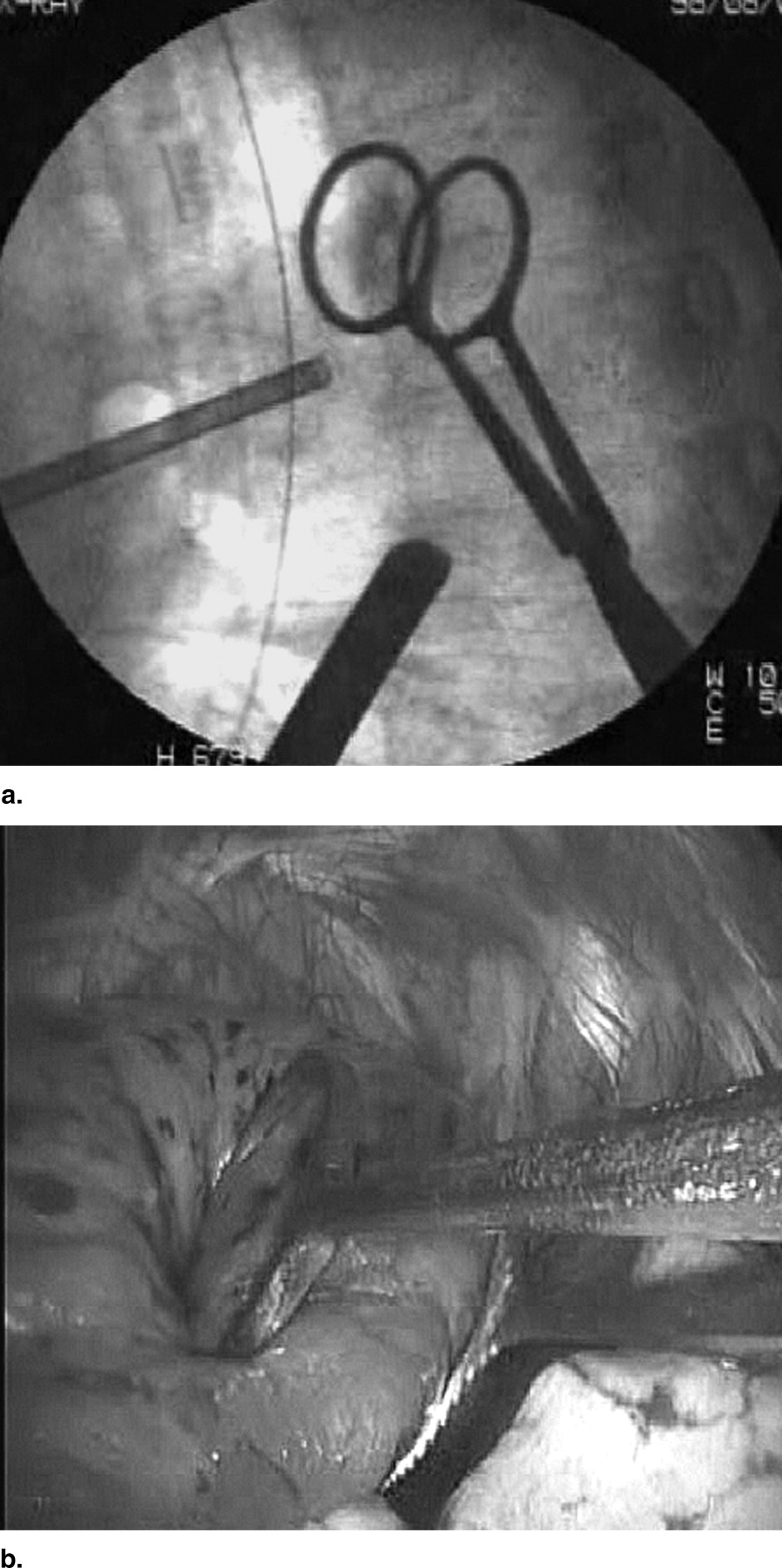
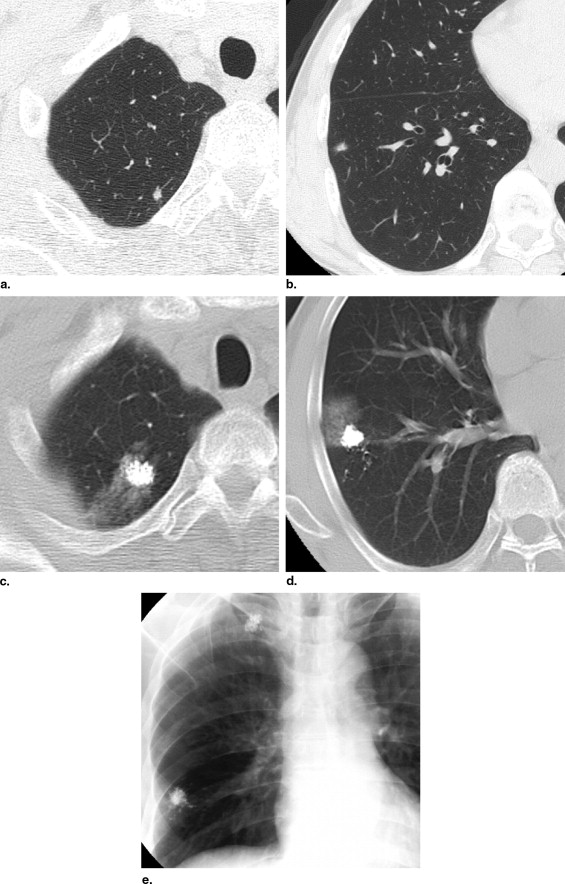
Lipiodol marking was performed under CT fluoroscopic guidance in 65 patients with 107 nodules. Of these, 65 (60.7%) were nodules with ground-glass opacity, and 42 were solid nodules on CT images. All nodules were marked with 0.3 to 0.5 mL lipiodol under CT fluoroscopic guidance 1 or 3 days before or on the day of surgery. At surgery, marked nodules were grasped with ring-shaped forceps under a C-arm fluoroscope and resected. Postoperatively, all 55 patients with malignant tumors ( n = 78) were followed by computed tomography at 3-month intervals to detect needle tract or pleural recurrence.
Results
All 107 nodules were marked with lipiodol; under the C-arm fluoroscope, they appeared as radiopaque spots. On postprocedural computed tomography, pneumothorax occurred in 20 patients (31%); its incidence was higher in patients with lung emphysema surrounding the nodules ( P = .09), three of whom required tube drainage. Computed tomography detected pulmonary hemorrhage in 10 patients (15%); it was more frequent in patients with deep than shallow nodules (≥6 cm from the pleural surface and <6 cm from the pleural surface, respectively; P = .04). No patients presented with recurrence in needle tracts or on the pleural surface during a median postoperative follow-up of 14 months.
Conclusion
Lipiodol marking under CT fluoroscopic guidance is a useful and safe procedure for the intraoperative localization of ground-glass opaque and/or small, deep, solid nodules.
With advances in high-resolution computed tomography, the detection of small and ground-glass opaque (GGO) pulmonary nodules has increased. Because percutaneous or transbronchial biopsy of these lesions is often difficult, thoracoscopic surgical techniques have been used in diagnostic excisional biopsies and therapeutic resection procedures. The complete resection of nodules diagnosed by percutaneous needle biopsy can be difficult because they cannot be easily located by palpation. Therefore, marking techniques have been developed for their localization during thoracoscopic surgery; these include dye ( ), barium ( ), and contrast marking and the use of microcoils ( ), hook wires ( ), and contrast material ( ).
Traditional dye methods has drawbacks due to the rapid diffusion of injected dye around lung tissues. To enable dye detection, marking has to be performed within 3 hours of thoracoscopy; this requires the simultaneous availability of a computed tomographic (CT) scanner and an operating room. Furthermore, the injection site is blurred because of dye diffusion. Barium marking with CT bronchoscopy is also complicated because it necessitates the simultaneous use of bronchoscopic and CT instrumentation, and the marking of a single nodule takes approximately 30 minutes (range, 15–60) ( ). In addition, barium can mimic lesions on hematoxylin-eosin-stained sections, and it can induce inflammatory changes in lung tissue, rendering a histologic diagnosis difficult. Marking with microcoils also complicates histologic diagnoses because it leads to the destruction of nodules. In addition, it is rather expensive, costing approximately $150 per nodule in Japan. Because the hook-wire technique has been reported to produce massive air embolism ( ), it is prohibited in Japan.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Materials and methods
Get Radiology Tree app to read full this article<
Patients
Get Radiology Tree app to read full this article<
Table 1
Characteristics of the 65 Patients
Variable Value Age (y) 64 ± 12 (15–81) Men 36 Women 29 Emphysematous lung tissue around a nodule ( n = 65) Yes 14 No 51
Data are expressed as mean ± standard deviation (range) or number.
Table 2
Characteristics of the 107 Nodules
GGO Nodules Solid Nodules Variable (n = 65) (n = 42) Size (cm) (range) 0.9 ± 0.6 (0.3–2.7) 0.9 ± 0.5 (0.3–2.2) Distance from the pleura (range) 1.5 ± 1.1 (0.2–5.4) 1.4 ± 1.2 (0.2–4.4) Location (lobe) Right upper 17 10 Right middle 1 5 Right lower 15 11 Left upper 18 11 Left lower 14 5 Total 65 42
Data are expressed as mean ± standard deviation (range) or number.
Get Radiology Tree app to read full this article<
Marking Technique
Get Radiology Tree app to read full this article<

Get Radiology Tree app to read full this article<
Resection Technique
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Assessment of Localization
Get Radiology Tree app to read full this article<
Postoperative Follow-Up
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Table 3
Pathological Diagnoses of the 107 Nodules
Diagnosis_n_ Malignant ( n = 78) Atypical adenomatous hyperplasia 13 Bronchioloalveolar carcinoma 37 Adenocarcinoma 3 Squamous cell carcinoma 1 Small cell carcinoma 1 Carcinoid 1 Metastatic lung cancer 22 Benign ( n = 29) Old inflammation 13 Intrapulmonary lymphatic tissue 7 Granuloma 3 Arteriovenous malformation 2 Hamartoma 2 Sclerosing hemangioma 1 Amyloidosis 1
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 4
Complications After Lipiodol Marking
Complication Number of Patients (%)P Value Pneumothorax Emphysematous lung around a nodule 0.09 Yes 7/14 (50) No 13/51 (25) Frequency of needle insertion 0.41 Once 8/31 (26) More than twice 12/34 (35) Depth of needle insertion (cm) 0.41 <6 8/31 (26) >6 12/34 (35) Pulmonary hemorrhage Frequency of needle insertion 0.22 Once 3/31 (10) More than twice 7/34 (21) Distance of needle insertion (cm) 0.04 <6 2/31 (6) >6 8/34 (24)
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Kerrigan D.C., Spence P.A., Crittenden M.D., et. al.: Methylene blue guidance for simplified resection of a lung lesion. Ann Thorac Surg 1992; 53: pp. 163-164.
2. Endo M., Kotani Y., Satouchi M., et. al.: CT fluoroscopy-guided bronchoscopic dye marking for resection of small peripheral pulmonary nodules. Chest 2004; 125: pp. 1747-1752.
3. Shah R.M., Spirn P.W., Salazar A.M., et. al.: Localization of peripheral pulmonary nodules for thoracoscopic excision: value of CT-guided wire placement. AJR Am J Roentgenol 1993; 161: pp. 279-283.
4. Asano F., Matsuno Y., Ibuka T., et. al.: A barium marking method using an ultrathin bronchoscope with virtual bronchoscopic navigation. Respirology 2004; 9: pp. 409-413.
5. Okumura T., Kondo H., Suzuki K., et. al.: Fluoroscopy-assisted thoracoscopic surgery after computed tomography-guided bronchoscopic barium marking. Ann Thorac Surg 2001; 71: pp. 439-444.
6. Powel T.I., Jangra D., Clifton J.C., et. al.: Peripheral lung nodules: fluoroscopically guided video-assisted thoracoscopic resection after computed tomography-guided localization using platinum microcoils. Ann Surg 2004; 240: pp. 481-489.
7. Dendo S., Kanazawa S., Ando A., et. al.: Preoperative localization of small pulmonary lesions with a short hook wire and suture system: experience with 168 procedures. Radiology 2002; 225: pp. 511-518.
8. Wicky S., Dusmet M., Doenz F., et. al.: Computed tomography-guided localization of small lung nodules before video-assisted resection: experience with an efficient hook-wire system. J Thorac Cardiovasc Surg 2002; 124: pp. 401-403.
9. Nomori H., Horio H., Naruke T., et. al.: Fluoroscopy-assisted thoracoscopic resection of lung nodules marked with lipiodol. Ann Thorac Surg 2002; 74: pp. 170-173.
10. Moon S.W., Wang Y.P., Jo K.H., et. al.: Fluoroscopy-aided thoracoscopic resection of pulmonary nodule localized with contrast media. Ann Thorac Surg 1999; 68: pp. 1815-1820.
11. Watanabe K., Nomori H., Ohtsuka T., Kaji M., Naruke T., Suemasu K.: Usefulness and complications of computed tomography-guided lipiodol marking for fluoroscopy-assisted thoracoscopic resection of small pulmonary nodules: experience with 174 nodules. J Thorac Cardiovasc Surg 2006; 32: pp. 320-324.
12. Kamiyoshihara M., Sakata K., Ishikawa S., et. al.: Cerebral arterial air embolism following CT-guided lung needle marking. J Cardiovasc Surg (Torino) 2001; 42: pp. 699-700.
13. Horan T.A., Pinheiro P.M., Araujo L.M., et. al.: Massive gas embolism during pulmonary nodule hook wire localization. Ann Thorac Surg 2002; 73: pp. 1647-1649.
14. Sakiyama S., Kondo K., Matsuoka H., et. al.: Fatal air embolism during computed tomography-guided pulmonary marking with a hook-type marker. J Thorac Cardiovasc Surg 2003; 126: pp. 1207-1209.
15. Sato K., Miyauchi K., Shikata F., et. al.: Arterial air embolism during percutaneous pulmonary marking under computed tomography guidance. Jpn J Thorac Cardiovasc Surg 2005; 53: pp. 404-406.
16. Ohi S., Itoh Y., Neyatani H., et. al.: Air embolism following computed tomography-guided lung needle marking. Kyobu Geka 2004; 57: pp. 421-423.
17. Katada K., Kato R., Anno H., et. al.: Guidance with real-time CT fluoroscopy: early clinical experience. Radiology 1996; 200: pp. 851-856.
18. Sakiyama S., Kondo K., Matsuoka H., et. al.: Fatal air embolism during computed tomography-guided pulmonary marking with a hook-type marker. J Thorac Cardiovasc Surg 2003; 126: pp. 1207-1209.
19. Sinner W.N., Zajicek J.: Implantation metastasis after percutaneous transthoracic needle aspiration biopsy. Acta Radiol Diagn (Stockholm) 1976; 17: pp. 473-480.
20. Sawabata N., Ohta M., Maeda H.: Fine-needle aspiration cytologic technique for lung cancer has a high potential of malignant cell spread through the tract. Chest 2000; 118: pp. 936-939.
21. Berger R.L., Dargan E.L., Huang B.L.: Dissemination of cancer cells by needle biopsy of the lung. J Thorac Cardiovasc Surg 1972; 63: pp. 430-432.
22. Matsuguma H., Nakahara R., Kondo T., Kamiyama Y., Mori K., Yokoi K.: Risk of pleural recurrence after needle biopsy in patients with resected early stage lung cancer. Ann Thorac Surg 2005; 80: pp. 2026-2031.