
Rationale and Objectives
The optimal phase for the measurement of the aortic annular area for transcatheter aortic valve replacement (TAVR) is not standardized, although most agree that systolic measurements are preferred, when the annulus is larger. We hypothesized that the maximum annular area occurs at the cardiac phase of the maximum aortic valve opening (MAVO) and that this phase can be accurately and reproducibly assessed by visual inspection only.
Materials and Methods
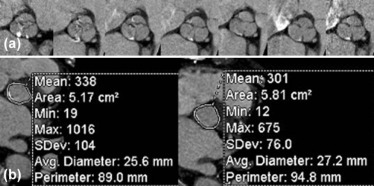
The aortic valve opening area was inspected visually by two readers to determine the MAVO phase. The annular area was measured at the MAVO phase and the typical systolic phase (35% of the R-R interval). Differences in the annular area that would change valve sizing for prostheses were noted.
Results
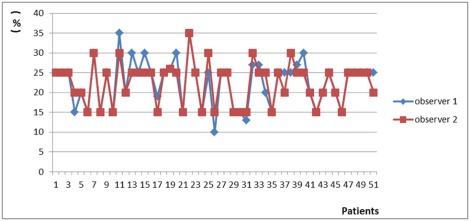
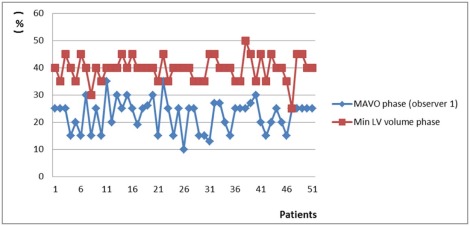
Fifty patients (mean age 81) were studied. Ninety percent had the MAVO at the 15%–25% R-R interval. There was high interobserver correlation (0.89) for determining the MAVO phase by visual inspection. For 49 out of 50 patients, the annular area was maximal at the MAVO phase. The mean difference in the annular area between the MAVO phase and 35% was 22.3 (±4.57) mm 2 . In 12% of the patients, the difference in the annular area changed the recommended size of a self-expanding prosthesis and would have altered the procedure in 32% for balloon-expandable prostheses.
Conclusions
Visually assessed MAVO occurs in early systole for most patients and is almost always the cardiac phase of the maximal aortic annular area. This method allows rapid and reproducible determination of the appropriate phase for TAVR planning measurements. Consideration should be given to optimizing pre-TAVR computed tomography acquisitions for early systolic reconstruction and visual determination of the MAVO.
Introduction
Transcatheter aortic valve replacement (TAVR) is an alternative to surgical aortic valve replacement in selected patients, including patients with symptomatic aortic stenosis who are not considered to be suitable candidates for surgery . Because the size of the annulus varies with the phase of the cardiac cycle , accurate assessment of the aortic annulus is a critical step in the planning of TAVR for sizing and determining patient eligibility because it enables proper valve sizing, grading calcification of the aortic annulus, and measurement of the distance to the coronaries’ origin. Concerning computed tomography (CT) protocols for annular assessment in TAVR patients, guidelines issued by the Society of Cardiovascular Computed Tomography in 2012 provide useful recommendations for data acquisition in this setting . The guidelines describe that the aortic root acquisition is performed during suspended respiration with either a “prospective” or a “retrospective ECG-gating with tube current modulation,” and a reconstructed slice thickness of less than 1 mm. However, specific protocols will vary depending on the institution and available scanner platform. Importantly, if multiphase data are available, systolic images are utilized for annular measurements as prior studies have demonstrated larger annular dimensions during systole. The change in annular dimensions during the cardiac cycle appears predominantly to affect annular area and short axis diameter measurements as annular configuration becomes less eccentric during systole. The annulus size increases in systole by 6%–13% with calcified valves, which applies in most TAVR cases . Therefore, even though the Society of Cardiovascular Computed Tomography guidelines do not mandate multiphase reconstructions for a pre-TAVR computed tomography angiogram (CTA) , most institutions do obtain these data by performing a retrospectively gated CTA.
At which specific systolic phase is the annulus maximal in size? Possibilities include end systole when the left ventricular (LV) volume is minimal or when the aortic valve opening is maximal. Although the consensus is to use a systolic phase because the annulus is larger, the specific phase of the cardiac cycle for optimal measurement of the annular area is not standardized , and there is no guideline to determine the best phase for annular measurement to avoid postprocedural paravalvular regurgitation or aortic annulus injury. Specifically, there is no consensus on the optimal systolic phase for TAVR planning. One approach is a fixed percentage of the R-R interval, for example, 30%–35% for systole and 65%–70% for diastole , with one study showing that the physiological systolic phase was more likely 40%–50% of the R-R interval, at which point the LV volume is minimal . There is a need to standardize the measurement protocol for TAVR, and an optimal method for measurement should be chosen that is universally used to size prosthetic valves for TAVR. In our practice, we noticed that the phase of the maximum aortic valve opening (MAVO) was not always identical to the phase of the minimal LV volume in patients with stenotic valves and was seen earlier than both 30%–35% and 40%–50% of the cardiac cycle.
Get Radiology Tree app to read full this article<
Materials and Methods
Get Radiology Tree app to read full this article<
Identification of the MAVO Phase and the Annular Size Measurement
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Interobserver Variability
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Conclusions
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Kodali S.K., Williams M.R., Smith C.R., et. al.: Two-year outcomes after transcatheter or surgical aortic-valve replacement. N Engl J Med 2012; 366: pp. 1686-1695.
2. Makkar R.R., Fontana G.P., Jilaihawi H., et. al.: Transcatheter aortic-valve replacement for inoperable severe aortic stenosis. N Engl J Med 2012; 366: pp. 1696-1704.
3. Lehmkuhl L., Foldyna B., Von Aspern K., et. al.: Inter-individual variance and cardiac cycle dependency of aortic root dimensions and shape as assessed by ECG-gated multi-slice computed tomography in patients with severe aortic stenosis prior to transcatheter aortic valve implantation: is it crucial for correct sizing?. Int J Cardiovasc Imaging 2013; 29: pp. 693-703.
4. de Heer L.M., Budde R.P., Mali W.P., et. al.: Aortic root dimension changes during systole and diastole: evaluation with ECG-gated multidetector row computed tomography. Int J Cardiovasc Imaging 2011; 27: pp. 1195-1204.
5. Bertaso A.G., Wong D.T., Liew G.Y., et. al.: Aortic annulus dimension assessment by computed tomography for transcatheter aortic valve implantation: differences between systole and diastole. Int J Cardiovasc Imaging 2012; 28: pp. 2091-2098.
6. Leipsic J., Gurvitch R., Labounty T.M., et. al.: Multidetector computed tomography in transcatheter aortic valve implantation. JACC Cardiovasc Imaging 2011; 4: pp. 416-429.
7. Holmes D.R., Mack M.J., Kaul S., et. al.: 2012 ACCF/AATS/SCAI/STS expert consensus document on transcatheter aortic valve replacement. J Am Coll Cardiol 2012; 59: pp. 1200-1254.
8. Achenbach S., Delgado V., Hausleiter J., et. al.: SCCT expert consensus document on computed tomography imaging before transcatheter aortic valve implantation (TAVI)/transcatheter aortic valve replacement (TAVR). J Cardiovasc Comput Tomogr 2012; 6: pp. 366-380.
9. Hamdan A., Guetta V., Konen E., et. al.: Deformation dynamics and mechanical properties of the aortic annulus by 4-dimensional computed tomography: insights into the functional anatomy of the aortic valve complex and implications for transcatheter aortic valve therapy. J Am Coll Cardiol 2012; 59: pp. 119-127.
10. Lehmkuhl L., Foldyna B., Haensig M., et. al.: Role of preprocedural computed tomography in transcatheter aortic valve implantation. Rofo 2013; 185: pp. 941-949.
11. Feuchtner G.M., Dichtl W., Friedrich G.J., et. al.: Multislice computed tomography for detection of patients with aortic valve stenosis and quantification of severity. J Am Coll Cardiol 2006; 47: pp. 1410-1417.
12. Kasel A.M., Cassese S., Bleiziffer S., et. al.: Standardized imaging for aortic annular sizing: implications for transcatheter valve selection. JACC Cardiovasc Imaging 2013; 6: pp. 249-262.
13. Blanke P., Russe M., Leipsic J., et. al.: Conformational pulsatile changes of the aortic annulus: impact on prosthesis sizing by computed tomography for transcatheter aortic valve replacement. JACC Cardiovasc Interv 2012; 5: pp. 984-994.
14. Willson A.B., Webb J.G., Freeman M., et. al.: Computed tomography-based sizing recommendations for transcatheter aortic valve replacement with balloon-expandable valves: comparison with transesophageal echocardiography and rationale for implementation in a prospective trial. J Cardiovasc Comput Tomogr 2012; 6: pp. 406-414.
15. Gurvitch R., Webb J.G., Yuan R., et. al.: Aortic annulus diameter determination by multidetector computed tomography: reproducibility, applicability, and implications for transcatheter aortic valve implantation. JACC Cardiovasc Interv 2011; 4: pp. 1235-1245.
16. Willson A.B., Webb J.G., Labounty T.M., et. al.: 3-Dimensional aortic annular assessment by multidetector computed tomography predicts moderate or severe paravalvular regurgitation after transcatheter aortic valve replacement: a multicenter retrospective analysis. J Am Coll Cardiol 2012; 59: pp. 1287-1294.
17. Binder R.K., Webb J.G., Willson A.B., et. al.: The impact of integration of a multidetector computed tomography annulus area sizing algorithm on outcomes of transcatheter aortic valve replacement: a prospective, multicenter, controlled trial. J Am Coll Cardiol 2013; 62: pp. 431-438.
18. Vahanian A., Alfieri O., Al-Attar N., et. al.: Transcatheter valve implantation for patients with aortic stenosis: a position statement from the European association of cardio-thoracic surgery (EACTS) and the European Society of Cardiology (ESC), in collaboration with the European Association of Percutaneous Cardiovascular Interventions (EAPCI). EuroIntervention 2008; 4: pp. 193-199.
19. Tops L.F., Wood D.A., Delgado V., et. al.: Noninvasive evaluation of the aortic root with multislice computed tomography implications for transcatheter aortic valve replacement. JACC Cardiovasc Imaging 2008; 1: pp. 321-330.
20. Wood D.A., Tops L.F., Mayo J.R., et. al.: Role of multislice computed tomography in transcatheter aortic valve replacement. Am J Cardiol 2009; 103: pp. 1295-1301.
21. Detaint D., Lepage L., Himbert D., et. al.: Determinants of significant paravalvular regurgitation after transcatheter aortic valve: implantation impact of device and annulus discongruence. JACC Cardiovasc Interv 2009; 2: pp. 821-827.
22. Tay E.L., Gurvitch R., Wijeysinghe N., et. al.: Outcome of patients after transcatheter aortic valve embolization. JACC Cardiovasc Interv 2011; 4: pp. 228-234.
23. Blanke P., Reinohl J., Schlensak C., et. al.: Prosthesis oversizing in balloon-expandable transcatheter aortic valve implantation is associated with contained rupture of the aortic root. Circ Cardiovasc Interv 2012; 5: pp. 540-548.
24. Pasic M., Buz S., Dreysse S., et. al.: Transapical aortic valve implantation in 194 patients: problems, complications, and solutions. Ann Thorac Surg 2010; 90: pp. 1463-1469. discussion 9–70
25. Schultz C.J., Moelker A.D., Tzikas A., et. al.: Cardiac CT: necessary for precise sizing for transcatheter aortic implantation. EuroIntervention 2010; 6: pp. G6-G13.
26. Doddamani S., Grushko M.J., Makaryus A.N., et. al.: Demonstration of left ventricular outflow tract eccentricity by 64-slice multi-detector CT. Int J Cardiovasc Imaging 2009; 25: pp. 175-181.
27. Altiok E., Koos R., Schroder J., et. al.: Comparison of two-dimensional and three-dimensional imaging techniques for measurement of aortic annulus diameters before transcatheter aortic valve implantation. Heart 2011; 97: pp. 1578-1584.
28. Dashkevich A., Blanke P., Siepe M., et. al.: Preoperative assessment of aortic annulus dimensions: comparison of noninvasive and intraoperative measurement. Ann Thorac Surg 2011; 91: pp. 709-714.
29. Blanke P., Siepe M., Reinohl J., et. al.: Assessment of aortic annulus dimensions for Edwards SAPIEN Transapical Heart Valve implantation by computed tomography: calculating average diameter using a virtual ring method. Eur J Cardiothorac Surg 2010; 38: pp. 750-758.
30. Colli A., Nofrerias E.F., Escudero A.: Aortic root rupture during trans-catheter aortic valve implantation. Eur J Cardiothorac Surg 2011; 39: pp. 788.
31. Buzzatti N., Maisano F., Latib A., et. al.: Computed tomography-based evaluation of aortic annulus, prosthesis size and impact on early residual aortic regurgitation after transcatheter aortic valve implantation. Eur J Cardiothorac Surg 2013; 43: pp. 43-50. discussion 50–51
32. Jurencak T., Turek J., Kietselaer B.L., et. al.: MDCT evaluation of aortic root and aortic valve prior to TAVI. What is the optimal imaging time point in the cardiac cycle?. Eur Radiol 2015; 25: pp. 1975-1983.
33. Feuchtner G.M., Muller S., Bonatti J., et. al.: Sixty-four slice CT evaluation of aortic stenosis using planimetry of the aortic valve area. AJR Am J Roentgenol 2007; 189: pp. 197-203.