
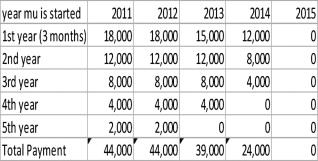
The benefits of an interactive online world have affected the way we purchase products and plan our vacations. It is only a matter of time before consumers start demanding health care with the same convenience that comes with booking an airline flight or managing a bank account. The health care industry itself requires periodic and mandatory data analysis for outcome analysis, clinical benchmarking, quality improvement, forming guidelines, and making decisions. The federal government and health care community have been working together to come up with more robust and cost-effective health care informatics solutions. Meaningful use (MU) intends to establish a new standard for health care informatics in the United States. The term “meaningful use” implies that health care information and technology systems not just exist, but also serve as an integral part of physician and hospital workflow; leading to cost savings as well as improved outcomes. Under this concept, the federal government is offering maximum incentive payments of up to $44,000 per physician (including radiologists) if they can meet all the requirements as laid down in the MU measures. Unfortunately, penalties will kick in if physicians are not compliant with MU by 2015. This will be done in at least three stages, with Stage 1 already in effect (as of January 3, 2011). This will be the first in a series of articles outlining MU and what is in store for radiology. We will go in depth about who is eligible, and how the payment schedule is set up. We will break down the core and menu set measures to suggest what can be excluded by most radiologists. We will also go through some case studies and examine what lies in store for radiology.
The benefits of an interactive online world are obvious to anyone who can book an airline ticket on a cell phone or call a friend by pressing a button on a car steering wheel. Despite our rapid adaptation of technology, patients still have to call doctors’ offices for appointments, call for imaging appointments, and use regular mail for correspondence between insurance companies and physicians. Even lack of online access to patient histories and other privacy concerns feel antiquated when contrasted with the success of online banking and finance.
Partially because of the belief that the health care information technology (HIT) industry was lagging behind the rest of the information technology (IT) sector, the federal government started looking at ways to stimulate both the development and implementation of HIT within the United States. The focus was on obtaining pieces of information that would not only be helpful for the individual physician in his or her practice, but also over time serve as a resource to better determine distribution of government funds and assets. An example of this would be to use data pooled from hospitals across the country to help determine how best to distribute vaccines across the country. Some other potential benefits of HIT include patient portals, better communication among consulting physicians, a more streamlined billing process, and a much improved scheduling workflow. It was this future vision for HIT in America that paved the way for meaningful use (MU) legislation.
MU is overseen by the Department of Health and Human Services. Two agencies, the Office of the National Coordinator for Health IT (ONC), and the Center for Medicare and Medicaid Services (CMS), work under the department of Health and Human Services (HHS) to develop and implement MU measures and criteria. The CMS works with physicians and attestation, whereas the ONC works with vendors and develops guidance for them to follow. The ONC, along with the National Institute for Standards and Technology (NIST) also developed ways to test products for MU certification. Third-party, private ONC-approved testing and certification bodies were then created to apply these tests. A vendor applies for MU certification to the approved testing and certification body, whereas a physician applies for certification to the CMS.
Contrary to popular belief, MU funds were allocated in the stimulus bill as part of the American Recovery and Reinvestment Act of 2009 before passage of the health care reform bill in 2010. Therefore, the program will not be affected by a repeal of the Patient Protection and Affordable Care act of 2010 (ie, The Healthcare Reform Bill) .
MU is divided into an eligible hospital (EH) program and an eligible professional (EP) program. There is also a separate Medicaid version. This article tackles MU from an eligible professional standpoint through Medicare, because that is what most radiologists will qualify for.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Who is eligible?
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Payment and penalties schedule
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Meaningful use measures
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Fifteen Core Objectives
Get Radiology Tree app to read full this article<
Table 1
Core Set at a Glance: A Summary of the Features of Core Set with a Suggestion for Potential Ease of Adoption by Radiologists
Core Measures Ease of Adoption by RIS as a Certified EHR Module Clinician physician order entry for medication orders Probably excluded Generate and transmit E-prescriptions Probably excluded Record vital signs, height, weight, blood pressure. Calculate BMI Probably excluded Provide patients with an electronic copy of their information within 3 business days Probably already adopted Record patient demographic information Probably already adopted Provide clinical summary for each office visit Probably already adopted Recording smoking status for anyone age 13 years or older Could be implemented easily Active allergy list Could be implemented easily Active medication list Might be difficult to maintain up-to-date list Implement drug-drug and drug allergy interaction checks Probably easy to adopt Maintain an active problem list of current and active diagnosis Might be difficult to maintain up-to-date list Protect electronic health information created or maintained by the certified EHR technology Probably no mechanism in current RIS/PACS to support this. Capability to exchange key clinical information among providers of care and patients authorized entities May be possible Implement one clinical decision support rule relevant to the specialty More than simple search function with RIS Clinical quality measures No mechanism for adoption. Will likely need a separate certified module
BMI, body mass index; HER, Electronic Health Record; RIS, Radiology Information Systems.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
There are 10 Menu Set Items; You Need to Pick 5
Get Radiology Tree app to read full this article<
Table 2
Menu Set at a Glance: A Summary of the Features of Menu Set with a Suggestion for Potential Ease of Adoption by Radiologists
Menu Set Measures Potential Ease of Adoption by Radiologists Using a RIS with Modular EHR Certification Medication reconciliation Probably excluded Summary of care record for each transition of care or referral Probably excluded Submission of electronic data to immunization registries Probably excluded Implement drug formulary checks Probably excluded Incorporate clinical lab test results into the EHR as structured data Probably excluded Capability to submit electronic syndromic surveillance data and actual submission according to applicable law and practice Probably excluded Use certified EHR technology to identify patient-specific education resources and provide those resources to patients if possible May conflict with clinicians Provide patients with timely electronic access to their health information (including lab results, problem list, medication lists, and allergies) within 4 business days of the information being available to the eligible physician May need a patient portal. Outside the purview of radiologists Send reminders to patients for preventive and/or follow-up care Very difficult to apply to 20% of all patients Generate lists of patients by specific conditions to use for quality improvements, reduction of disparities, research, or outreach Available as third-party options outside of PACS.
HER, Electronic Health Record; PACS, Picture Archiving and Communication System; RIS, Radiology Information Systems.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Case studies
Get Radiology Tree app to read full this article<
Case Study 1: Radiology Practice Employed by a Hospital with an EHR
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Case Study 2: Radiology Group without an EHR
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
What lies ahead for radiology?
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Conclusion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Department of Health and Human Services. CMS final rule for stage 1 of meaningful use. Available at: http://edocket.access.gpo.gov/2010/pdf/2010-17210.pdf . Accessed January 15, 2011.
2. ACR. ACR Summary CMS and ONC Stage 1 Meaningful Use Final Rules. Available at: http://www.acr.org/SecondaryMainMenuCategories/GR_Econ/Meaningful-Use-Resource-Center.aspx . Accessed July 28, 2011.
3. Tang P, Hripcak G. HIT Policy Committee Meaningful Use Workgroup (December 13, 2010). US Department of Health and Human Services. Available at: http://healthit.hhs.gov/portal/server.pt/gateway/PTARGS_0_0_6010_1814_17824_43/http%3B/wci-pubcontent/publish/onc/public_communities/_content/files/mu_recs_121310.ppt . Accessed February 28, 2011.
4. The Library of Congress. Bill summary and status, 111th Congress: HR04851. THOMAS. Available at: http://thomas.loc.gov/cgi-bin/bdquery/z?d111:HR04851 . Accessed September 1, 2011.
5. Department of Health and Human Services. Eligibility requirement for professionals. Available at: http://www.cms.gov/EHRIncentivePrograms/15_Eligibility.asp#BOOKMARK1 . Accessed September 1, 2011.
6. CMS. Timeline, CMS Medicare and Medicaid EHR Incentive Programs Milestone. Available at: https://www.cms.gov/EHRIncentivePrograms/Downloads/EHRIncentProgtimeline508V1.pdf . Accessed September 1, 2011.
7. CMS. Center for medicare and medicaid. CMS finalizes requirements for the Medicare Electronic Health Records (EHR) incentive program. Available at: http://www.cms.gov/apps/media/press/factsheet.asp?Counter=3792&intNumPerPage=10&checkDate=&checkKey=&srchType=1&numDays=3500&srchOpt=0&srchData=&keywordType=All&chkNewsType=6&intPage=&showAll=&pYear=&year=&desc=&cboOrder=date . Accessed September 1, 2011.
8. Blumenthal D., Tavenner M.: The ‘meaningful use’ regulation for electronic health records. New Engl J Med 2010; 363: pp. 501-504.
9. Department of Health and Human Services. Overview of eligible core and menu set objectives. Available at: https://www.cms.gov/EHRIncentivePrograms/Downloads/EP-MU-TOC.pdf . Accessed September 1, 2011.
10. Meaningful Use Workgroup. Meaningful Use Workgroup request for comments regarding Stage 2 meaningful use (January 18, 2011). Available at: http://healthit.hhs.gov/media/faca/MU_RFC%20_2011-01-12_final.pdf . Accessed September 1, 2011.
11. ACR. ACR comments on MU workgroup RFC. Available at: http://www.acr.org/SecondaryMainMenuCategories/GR_Econ/FeaturedCategories/federal/hhs/ACR-Comments-to-the-Meaningful-Use-Workgroup–Draft-Advice-for-Stage-2-MU.aspx . Accessed September 1, 2011.
12. Flanders E.: The real “meaning” behind meaningful use. Radiographics 2010; 30: pp. 1329-1333.
13. Boland M.V.: Meaningful use of electronic health records in ophthalmology. Ophthalmology 2010; 117: pp. 2239-2240.
14. ACR. Meaningful Use of Certified EHR Technology for the Radiology Speciality (October 26, 2009). Available at: http://www.acr.org/SecondaryMainMenuCategories/GR_Econ/FeaturedCategories/federal/hhs/ACRCommentstotheHHSHITPolicyCommitteeMeaningfulUsePart2.aspx . Accessed September 1, 2011.