
Rational and Objectives
Microwave ablation is an alternative therapy with high cost-effectiveness for liver malignancy. The authors designed this experiment to compare the effect of microwave ablation using a non-internally cooled (NIC) antenna with that using an internally cooled (IC) antenna in both an ex vivo and an in vivo liver models.
Materials and Methods
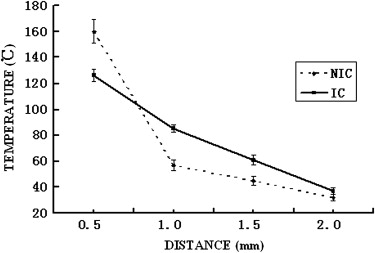
Sixty-two microwave ablations were performed in ex vivo porcine and in vivo canine liver models (NIC antenna, 28 coagulations; IC antenna, 34 coagulations). Pair comparisons were executed in terms of the coagulation parameters, including short-axis diameter (SD), long-axis diameter (LD), and spherical ratio (SR, SD/LD). The distributions of tissue temperatures were compared in ex vivo ablation. During in vivo ablation, the temperatures of antenna shaft were measured and unintended tissue coagulation were observed and compared.
Results
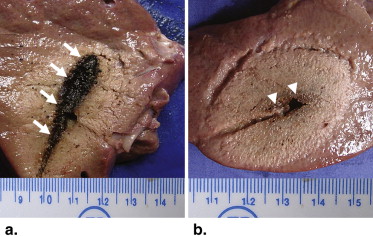
In both ex vivo and in vivo ablations, less charring areas were found around the IC antenna shaft. With a longer SD ( P < .01) and a shorter LD ( P < .01), the coagulations of IC antenna appeared to be more spherical than those of NIC antenna ( P < .01). During ablations in vivo, the temperatures of NIC antennas shaft were up to 90°C or even higher, which resulted in some unintended tissue coagulation, whereas the temperatures of IC antennas shaft were lower than 20°C in all ablation processes without any unintended tissue coagulation ( P < .01).
Conclusion
The IC antenna performed better than NIC antenna in microwave ablation for liver models and might be more suitable for therapy for liver malignancy in clinical practice.
Thermal ablation techniques, such as radiofrequency (RF) and microwave ablation , have been widely used as minimally invasive strategies to treat liver malignant tumors. So far, among all the thermal ablation modalities, RF is the most commonly modality adopted and reported, and significant advances have been work out recently, such as the use of multiprobe , multitined expandable , internally cooled (IC) , and perfusion RF electrodes . Microwave ablation, as a minimally invasive and high cost-effective modality, has been mainly used in Asia . RF ablation and microwave ablation have equivalent therapeutic effects, complication rates, local recurrence rates, and residual cancer rates. However, RF tumor ablation can be achieved with fewer sessions than microwave ablation, which may be attributed to the limitation of the small extent of coagulation necrosis produced with a single microwave application.
Theoretically, microwave ablation is more efficient than RF ablation because microwaves can penetrate more deeply than RF waves do and the delivery of microwave energy depends less on tissue texture and impedance . Microwave ablations were reported to be less affected by the heat-sink effect, which was believed to result in local recurrence . Recently, microwave ablation effect has been improved with the advent of triaxial antennas , loop antenna , and IC antenna . The IC antenna might be a promising one because it could increase microwave delivery, enlarge the ablation zone, and minimize collateral damages such as skin burn .
Get Radiology Tree app to read full this article<
Materials and methods
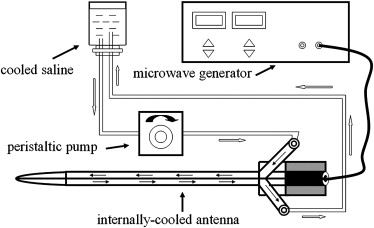
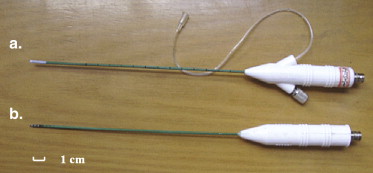
Microwave Ablation System
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Overall Study Design
Get Radiology Tree app to read full this article<
Ex Vivo Porcine Liver Ablation
Get Radiology Tree app to read full this article<
In Vivo Canine Liver Ablation
Get Radiology Tree app to read full this article<
Pathologic Studies
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Results
Ex Vivo Porcine Liver Ablation
Get Radiology Tree app to read full this article<
Table 1
Coagulation Diameters and Sphericity Index for Selected Treatment Duration and Power Settings in ex vivo Porcine Liver Ablation
NIC Antenna IC Antenna SD ∗ LD ∗ SR ∗ SD ∗ LD ∗ SR ∗ 30W 6 minutes 19 48 0.40 24 38 O.63 30W 8 minutes 22 49 0.45 27 44 0.61 30W 10 minutes 26 55 0.47 30 43 0.70 30W 12 minutes 28 58 0.48 34 40 0.85 30W 14 minutes 30 60 0.50 40 46 0.87 30W 16 minutes 35 63 0.56 43 45 0.96 40W 6 minutes 20 50 0.40 25 35 0.71 40W 8 minutes 25 54 0.46 30 42 0.71 40W 10 minutes 28 55 0.51 32 45 0.71 40W 12 minutes 31 60 0.52 34 50 0.68 40W 14 minutes 34 60 0.57 39 48 0.81 40W 16 minutes 41 65 0.63 42 50 0.84 50W 6 minutes 26 55 0.47 27 50 0.54 50W 8 minutes 28 58 0.48 34 50 0.68 50W 10 minutes NA NA NA 37 50 0.74 50W 12 minutes NA NA NA 39 50 0.78 50W 14 minutes NA NA NA 43 53 0.81 50W 16 minutes NA NA NA 45 55 0.82
NIC, non-internally cooled; IC, internally cooled; SD, short-axis diameter; LD, long-axis diameter (mm); SR, sphericity ratio; NA, not available, because the NIC antenna failed for any duration with the power higher than 60W or when the durations are longer than 9 minutes with the power of 50W. The four-pair data in both groups were excluded from paired Student t -test.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
In Vivo Canine Liver Ablation
Get Radiology Tree app to read full this article<
Table 2
Coagulation Diameters and Sphericity Index for Selected Treatment Duration and Power Settings in vivo Canine Liver Ablation
NIC Antenna IC Antenna SD ∗ LD ∗ SR ∗ SD ∗ LD ∗ SR ∗ 30W 5 minutes 17 35 0.49 19 24 0.79 30W 10 minutes 18 37 0.49 21 27 0.78 30W 15 minutes 20 41 0.49 23 35 0.66 30W 20 minutes 19 43 0.44 24 38 0.63 40W 5 minutes 22 36 0.61 21 31 0.68 40W 10 minutes 23 45 0.51 28 30 0.93 40W 15 minutes 22 32 0.69 29 35 0.83 40W 20 minutes 25 48 0.52 33 47 0.70 50W 5 minutes 18 46 0.39 22 36 0.61 50W 10 minutes 26 55 0.47 29 40 0.73 50W 15 minutes 26 50 0.52 31 40 0.78 50W 20 minutes 27 43 0.63 32 45 0.71 60W 5 minutes 23 35 0.66 23 39 0.59 60W 10 minutes 30 55 0.55 31 45 0.69 60W 15 minutes NA NA NA 32 45 0.71 60W 20 minutes NA NA NA 35 50 0.70
NIC, non-internally cooled; IC, internally cooled; SD, short-axis diameter; LD, long-axis diameter (mm); SR, sphericity ratio; NA, not available, because the NIC antenna failed for any duration with the power higher than 70W or when the durations are longer than 12 minutes with the power of 60W. The two-pair data in both groups were excluded from paired Student t -test.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
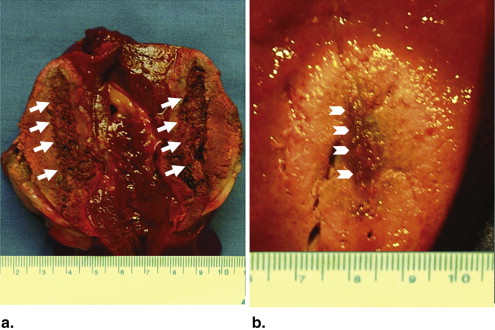
Pathology Results
Get Radiology Tree app to read full this article<
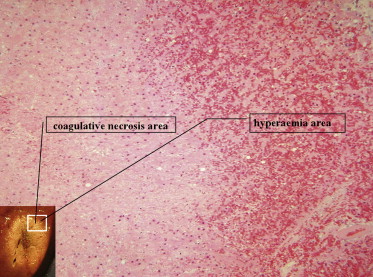
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Giorgio A., Tarantino L., de Stefano G., et. al.: Complications after percutaneous saline-enhanced radiofrequency ablation of liver tumors: 3-year experience with 336 patients at a single center. AJR Am J Roentgenol 2005; 184: pp. 207-211.
2. Shibata T., Shibata T., Maetani Y., et. al.: Radiofrequency ablation for small hepatocellular carcinoma: prospective comparison of internally cooled electrode and expandable electrode. Radiology 2006; 238: pp. 346-353.
3. Seror O., N’Kontchou G., Tin-Tin-Htar M., et. al.: Radiofrequency ablation with internally cooled versus perfused electrodes for the treatment of small hepatocellular carcinoma in patients with cirrhosis. J Vasc Interv Radiol 2008; 19: pp. 718-724.
4. Seki T., Wakabayashi M., Nakagawa T., et. al.: Ultrasonically guided percutaneous microwave coagulation therapy for small hepatocellular carcinoma. Cancer 1994; 74: pp. 817-825.
5. Lu M.D., Chen J.W., Xie X.Y., et. al.: Hepatocellular carcinoma: US-guided percutaneous microwave coagulation therapy. Radiology 2001; 221: pp. 167-172.
6. Itamoto T., Katayama K., Fukuda S., et. al.: Percutaneous microwave coagulation therapy for primary or recurrent hepatocellular carcinoma: long-term results. Hepatogastroenterology 2001; 48: pp. 1401-1405.
7. Dong B., Liang P., Yu X., et. al.: Percutaneous sonographically guided microwave coagulation therapy for hepatocellular carcinoma: results in 234 patients. AJR Am J Roentgenol 2003; 180: pp. 1547-1555.
8. Goldberg S.N., Gazelle G.S., Dawson S.L., et. al.: Tissue ablation with radiofrequency using multiprobe arrays. Acad Radiol 1995; 2: pp. 670-674.
9. Rossi S., Buscarini E., Garbagnati F., et. al.: Percutaneous treatment of small hepatic tumors by an expandable RF needle electrode. AJR Am J Roentgenol 1998; 170: pp. 1015-1022.
10. Shibata T., Iimuro Y., Yamamoto Y., et. al.: Small hepatocellular carcinoma: comparison of radio-frequency ablation and percutaneous microwave coagulation therapy. Radiology 2002; 223: pp. 331-337.
11. Ohmoto K., Yoshioka N., Tomiyama Y., et. al.: Radiofrequency ablation versus percutaneous microwave coagulation therapy for small hepatocellular carcinomas: a retrospective comparative study. Hepatogastroenterology 2007; 54: pp. 985-989.
12. Shock S.A., Meredith K., Warner T.F., et. al.: Microwave ablation with loop antenna: in vivo porcine liver model. Radiology 2004; 231: pp. 143-149.
13. Skinner M.G., Iizuka M.N., Kolios M.C., et. al.: A theoretical comparison of energy sources—microwave, ultrasound and laser—for interstitial thermal therapy. Phys Med Biol 1998; 43: pp. 3535-3547.
14. Wright A.S., Sampson L.A., Warner T.F., et. al.: Radiofrequency versus microwave ablation in a hepatic porcine model. Radiology 2005; 236: pp. 132-139.
15. Yu N.C., Raman S.S., Kim Y.J., et. al.: Microwave liver ablation: influence of hepatic vein size on heat-sink effect in a porcine model. J Vasc Interv Radiol 2008; 19: pp. 1087-1092.
16. Brace C.L., Laeseke P.F., Sampson L.A., et. al.: Microwave ablation with a single small-gauge triaxial antenna: in vivo porcine liver model. Radiology 2007; 242: pp. 435-440.
17. Yu N.C., Lu D.S., Raman S.S., et. al.: Hepatocellular carcinoma: microwave ablation with multiple straight and loop antenna clusters—pilot comparison with pathologic findings. Radiology 2006; 239: pp. 269-275.
18. Kuang M., Lu M.D., Xie X.Y., et. al.: Liver cancer: increased microwave delivery to ablation zone with cooled-shaft antenna—experimental and clinical studies. Radiology 2007; 242: pp. 914-924.
19. Wang Y., Sun Y., Feng L., et. al.: Internally cooled antenna for microwave ablation: results in ex vivo and in vivo porcine livers. Eur J Radiol 2008; 67: pp. 357-361.
20. Goldberg S.N., Grassi C.J., Cardella J.F., et. al.: Image-guided tumor ablation: standardization of terminology and reporting criteria. Radiology 2005; 235: pp. 728-739.
21. Burdio F., Navarro A., Berjano E.J., et. al.: Radiofrequency hepatic ablation with internally cooled electrodes and hybrid applicators with distant saline infusion using an in vivo porcine model. Eur J Surg Oncol 2008; 34: pp. 822-830.
22. Pereira P.L., Trubenbach J., Schenk M., et. al.: Radiofrequency ablation: in vivo comparison of four commercially available devices in pig livers. Radiology 2004; 232: pp. 482-490.
23. Seki T., Kubota Y., Wakabayashi M., et. al.: Percutaneous transhepatic microwave coagulation therapy for hepatocellular carcinoma proliferating in the bile duct. Dig Dis Sci 1994; 39: pp. 663-666.
24. Dong B.W., Liang P., Yu X.L., et. al.: Sonographically guided microwave coagulation treatment of liver cancer: an experimental and clinical study. AJR Am J Roentgenol 1998; 171: pp. 449-454.
25. Lorentzen T.: A cooled needle electrode for radiofrequency tissue ablation: thermodynamic aspects of improved performance compared with conventional needle design. Acad Radiol 1996; 3: pp. 556-563.
26. Lee J.M., Han J.K., Chang J.M., et. al.: Radiofrequency renal ablation: in vivo comparison of internally cooled, multitined expandable and internally cooled perfusion electrodes. J Vasc Interv Radiol 2006; 17: pp. 549-556.
27. Vogl T.J., Mack M.G., Roggan A., et. al.: Internally cooled power laser for MR-guided interstitial laser-induced thermotherapy of liver lesions: initial clinical results. Radiology 1998; 209: pp. 381-385.
28. Ritz J.P., Lehmann K.S., Mols A., et. al.: Laser-induced thermotherapy for lung tissue–evaluation of two different internally cooled application systems for clinical use. Lasers Med Sci 2008; 23: pp. 195-202.