
Rationale and Objectives
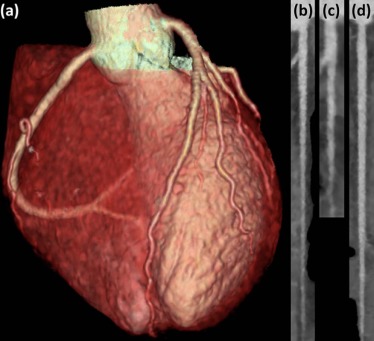
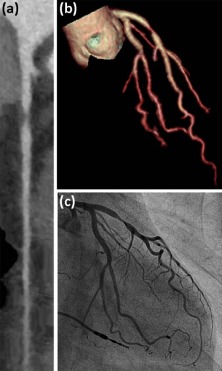
The aim of the study was to evaluate the impact of the latest coronary computed tomography angiography (CCTA) techniques allowing a radiation- and contrast-sparing protocol on image quality in unselected patients referred for exclusion of suspected coronary artery disease (CAD).
Materials and Methods
This prospective study was approved by the local ethics committee, and all patients provided written informed consent. Between March and June 2015, 89 consecutive patients (61% male; mean age 55 ± 11 years) referred for exclusion of CAD by 256-slice CCTA using prospective electrocardiogram triggering were included. Tube voltage (80–120 kVp), tube current (180–310 mA) as well contrast agent volume (25–45 mL) and flow rate (3.5–5 mL/s) were adapted to body mass index. Signal intensity was measured by placing a region of interest in the aortic root, the left main artery, and the proximal right coronary artery. Image noise was measured in the aortic root. Two independent blinded readers semi-quantitatively assessed the image quality regarding motion, noise, and contrast on a 4-point scale.
Results
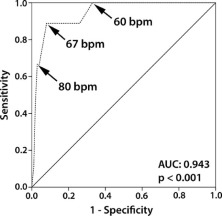
Median contrast agent volume and median effective radiation dose were 35 mL (interquartile range, 30–40 mL) and 0.5 mSv (interquartile range, 0.4–0.6 mSv), respectively. Mean attenuation in the aortic root was 412 ± 89 Hounsfield units. Diagnostic image quality was obtained in 1050 of 1067 (98.4%) coronary segments and, on an intention-to-diagnosis basis, in 85 of 89 (95.5%) patients. Below a cut-off heart rate of 67 beats/min, only 1 of 974 (0.1%) coronary segments was nondiagnostic.
Conclusion
A radiation- and contrast-sparing protocol for CCTA on a latest generation 256-slice computed tomography scanner yields diagnostic image quality in patients referred for CAD exclusion in daily clinical routine.
Introduction
Coronary computed tomography angiography (CCTA) has become an important and robust noninvasive imaging tool for the exclusion of significant coronary artery disease (CAD). However, its growing clinical use has raised concerns about the potential induction of malignancies due to the increased burden of radiation exposure for patients . Furthermore, the debate on the potential risks associated with cardiovascular imaging has recently been extended to additional components, and contrast agents have been identified as significant contributors of potential risk. In fact, the rate of death and serious acute adverse events due to contrast agent exposure is not negligible and outweighs the radiation-related risks . As a consequence, various technological advances have evolved not only to reduce radiation exposure , but also to save contrast agent volume , potentially enabling a CCTA imaging approach with a combined low radiation and low contrast agent volume exposure.
The introduction of prospective electrocardiogram (ECG) triggering , including its adaption to high-pitch helical scanning , has paved the way for a substantial reduction of radiation exposure from initially over 20 mSv with conventional helical acquisition to approximately 2 mSv in current daily clinical routine . Nevertheless, prospective triggering is prone to image quality degradation if the patient’s heart rate is irregular or high (ie >62 beats/min at a gantry rotation time of 350 ms) . Wide-volume 256-slice scanners with 16-cm cranial-caudal coverage and fast gantry rotation time of 280 ms permit acquisition of the whole heart within a single heartbeat, which not only eliminates misalignment artifacts , but also results in decreased radiation dose by precluding redundant radiation from overlapping of sequential axial scans and allows for a reduction of contrast agent volume because of shorter acquisition time . Furthermore, a more powerful X-ray generator enables acquisition at tube voltages of 100 kVp or below, thereby offering a further reduction of radiation dose, while yielding higher contrast than the standard 120 kVp technique because the X-ray output energy is closer to the iodine K-edge of 33 keV .
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Methods
Patient Population
Get Radiology Tree app to read full this article<
Image Acquisition
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 1
BMI-adapted Scan and Contrast Protocol
BMI (kg/m 2 ) Voltage (kV) Current (mA) Dose (mL) Flow Rate (mL/s) ≤20.0 80 180 25 3.5 20.1–22.4 100 180 30 4.0 22.5–24.9 100 215 30 4.0 25.0–27.4 100 270 35 4.5 27.5–29.9 100 310 40 5.0 ≥30.0 120 310 45 5.0
BMI, body mass index.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Quantitative Image Analysis
Get Radiology Tree app to read full this article<
Qualitative Image Analysis
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Results
Study Population
Get Radiology Tree app to read full this article<
Table 2
Patient Baseline Demographics ( n = 89)
Male Gender (%) 61 Age (years) Mean ± SD 55 ± 11 Range 27–78 Body mass index Median (kg/m 2 ) 26.1 Interquartile range (kg/m 2 ) 22.7–28.7 Minimum to maximum (kg/m 2 ) 17.8–45.2 BMI ≤ 20 kg/m 2 (%) 9 BMI = 20.1–22.4 kg/m 2 (%) 12 BMI = 22.5–24.9 kg/m 2 (%) 25 BMI = 25.0–27.4 kg/m 2 (%) 21 BMI = 27.5–29.9 kg/m 2 (%) 17 BMI ≥ 30.0 kg/m 2 (%) 16 Cardiovascular risk factors (%) Smoking 34 Diabetes mellitus 5 Hypertension 44 Dyslipidemia 43 Positive family history 29 Clinical symptoms (%) Typical angina pectoris 10 Atypical chest pain 43 Dyspnea 15 Asymptomatic 34
BMI, body mass index; SD, standard deviation.
Get Radiology Tree app to read full this article<
CCTA Parameters
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Quantitative Image Analysis
Get Radiology Tree app to read full this article<
Qualitative Image Analysis and Study Interpretability
Get Radiology Tree app to read full this article<
Table 3
Image Quality and Study Interpretability
Variable Segment Based Patient Based Motion Excellent (4.0) 907(85.0%) NA Good (3.0–3.9) 112(10.5%) NA Fair (2.0–2.9) 39(3.7%) NA Nondiagnostic (1.0–1.9) 9(0.8%) 6 (6.7%) Noise Excellent 644(60.4%) NA Good 293(27.5%) NA Fair 122(11.4%) NA Nondiagnostic 8(0.7%) 4 (4.5%) Contrast Excellent 644(60.4%) NA Good 349(32.7%) NA Fair 72(6.7%) NA Nondiagnostic 2(0.2%) 2 (2.2%) Total number 1067 89 Total number of interpretable segments/patients 98.4% 91%
Numbers are given, and percentages of total amount are in parentheses. NA, not applicable.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Determinates of Image Quality
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Acknowledgments
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Sodickson A., Baeyens P.F., Andriole K.P., et. al.: Recurrent CT, cumulative radiation exposure, and associated radiation-induced cancer risks from CT of adults. Radiology 2009; 251: pp. 175-184.
2. Knuuti J., Bengel F., Bax J.J., et. al.: Risks and benefits of cardiac imaging: an analysis of risks related to imaging for coronary artery disease. Eur Heart J 2014; 35: pp. 633-638.
3. Rubin G.D., Leipsic J., Joseph Schoepf U., et. al.: CT angiography after 20 years: a transformation in cardiovascular disease characterization continues to advance. Radiology 2014; 271: pp. 633-652.
4. Hein P.A., May J., Rogalla P., et. al.: Feasibility of contrast material volume reduction in coronary artery imaging using 320-slice volume CT. Eur Radiol 2010; 20: pp. 1337-1343.
5. Buechel R.R., Husmann L., Herzog B.A., et. al.: Low-dose computed tomography coronary angiography with prospective electrocardiogram triggering: feasibility in a large population. J Am Coll Cardiol 2011; 57: pp. 332-336.
6. Achenbach S., Marwan M., Ropers D., et. al.: Coronary computed tomography angiography with a consistent dose below 1 mSv using prospectively electrocardiogram-triggered high-pitch spiral acquisition. Eur Heart J 2010; 31: pp. 340-346.
7. Husmann L., Valenta I., Gaemperli O., et. al.: Feasibility of low-dose coronary CT angiography: first experience with prospective ECG-gating. Eur Heart J 2008; 29: pp. 191-197.
8. Hausleiter J., Meyer T., Hermann F., et. al.: Estimated radiation dose associated with cardiac CT angiography. JAMA 2009; 301: pp. 500-507.
9. Dewey M., Zimmermann E., Deissenrieder F., et. al.: Noninvasive coronary angiography by 320-row computed tomography with lower radiation exposure and maintained diagnostic accuracy: comparison of results with cardiac catheterization in a head-to-head pilot investigation. Circulation 2009; 120: pp. 867-875.
10. Hsiao E.M., Rybicki F.J., Steigner M.: CT coronary angiography: 256-slice and 320-detector row scanners. Curr Cardiol Rep 2010; 12: pp. 68-75.
11. Nakayama Y., Awai K., Funama Y., et. al.: Abdominal CT with low tube voltage: preliminary observations about radiation dose, contrast enhancement, image quality, and noise. Radiology 2005; 237: pp. 945-951.
12. Marin D., Nelson R.C., Schindera S.T., et. al.: Low-tube-voltage, high-tube-current multidetector abdominal CT: improved image quality and decreased radiation dose with adaptive statistical iterative reconstruction algorithm—initial clinical experience. Radiology 2010; 254: pp. 145-153.
13. Leipsic J., Labounty T.M., Heilbron B., et. al.: Estimated radiation dose reduction using adaptive statistical iterative reconstruction in coronary CT angiography: the ERASIR study. AJR Am J Roentgenol 2010; 195: pp. 655-660.
14. Husmann L., Herzog B.A., Burkhard N., et. al.: Low-dose coronary CT angiography with prospective ECG triggering: validation of a contrast material protocol adapted to body mass index. AJR Am J Roentgenol 2009; 193: pp. 802-806.
15. Ghadri J.R., Goetti R., Fiechter M., et. al.: Inter-scan variability of coronary artery calcium scoring assessed on 64-multidetector computed tomography vs. dual-source computed tomography: a head-to-head comparison. Eur Heart J 2011; 32: pp. 1865-1874.
16. Austen W.G., Edwards J.E., Frye R.L., et. al.: A reporting system on patients evaluated for coronary artery disease. Report of the Ad Hoc Committee for Grading of Coronary Artery Disease, Council on Cardiovascular Surgery, American Heart Association. Circulation 1975; 51: pp. 5-40.
17. Husmann L., Leschka S., Desbiolles L., et. al.: Coronary artery motion and cardiac phases: dependency on heart rate—implications for CT image reconstruction. Radiology 2007; 245: pp. 567-576.
18. Chen M.Y., Shanbhag S.M., Arai A.E.: Submillisievert median radiation dose for coronary angiography with a second-generation 320-detector row CT scanner in 107 consecutive patients. Radiology 2013; 267: pp. 76-85.
19. Achenbach S., Goroll T., Seltmann M., et. al.: Detection of coronary artery stenoses by low-dose, prospectively ECG-triggered, high-pitch spiral coronary CT angiography. JACC Cardiovasc Imaging 2011; 4: pp. 328-337.
20. Fuchs T.A., Stehli J., Bull S., et. al.: Coronary computed tomography angiography with model-based iterative reconstruction using a radiation exposure similar to chest X-ray examination. Eur Heart J 2014; 35: pp. 1131-1136.
21. Schuhbaeck A., Achenbach S., Layritz C., et. al.: Image quality of ultra-low radiation exposure coronary CT angiography with an effective dose <0.1 mSv using high-pitch spiral acquisition and raw data-based iterative reconstruction. Eur Radiol 2013; 23: pp. 597-606.
22. Oda S., Utsunomiya D., Yuki H., et. al.: Low contrast and radiation dose coronary CT angiography using a 320-row system and a refined contrast injection and timing method. J Cardiovasc Comput Tomogr 2015; 9: pp. 19-27.
23. Sun G., Hou Y.B., Zhang B., et. al.: Application of low tube voltage coronary CT angiography with low-dose iodine contrast agent in patients with a BMI of 26–30 kg/m 2 . Clin Radiol 2015; 70: pp. 138-145.
24. Qi L., Wu S.Y., Meinel F.G., et. al.: Prospectively ECG-triggered high-pitch 80 kVp coronary computed tomography angiography with 30 mL of 270 mg I/mL contrast material and iterative reconstruction. Acta Radiol 2016; 57: pp. 287-294.
25. Cademartiri F., Mollet N.R., van der Lugt A., et. al.: Intravenous contrast material administration at helical 16-detector row CT coronary angiography: effect of iodine concentration on vascular attenuation. Radiology 2005; 236: pp. 661-665.
26. Pazhenkottil A.P., Husmann L., Buechel R.R., et. al.: Validation of a new contrast material protocol adapted to body surface area for optimized low-dose CT coronary angiography with prospective ECG-triggering. Int J Cardiovasc Imaging 2010; 26: pp. 591-597.
27. Toprak O.: Conflicting and new risk factors for contrast induced nephropathy. J Urol 2007; 178: pp. 2277-2283.
28. Gruberg L., Mintz G.S., Mehran R., et. al.: The prognostic implications of further renal function deterioration within 48 h of interventional coronary procedures in patients with pre-existent chronic renal insufficiency. J Am Coll Cardiol 2000; 36: pp. 1542-1548.
29. Thomsen H.S.: Current evidence on prevention and management of contrast-induced nephropathy. Eur Radiol 2007; 17: pp. F33-F37.