
Rationale and Objectives
When using mammographic detectors of different sizes, it can be difficult to match patient breast size to optimal detector size. We studied whether a mismatch between breast size and optimal detector size resulted in increased radiation exposure.
Materials and Methods
All screening and diagnostic (Dx) mammography patients during a 6-week period in November–December 2009 (864 patients) were evaluated (institutional review board exemption for quality assurance studies). Data gathered included breast size (large or small), detector size used, number of views obtained, mean glandular dose (MGD) per breast, and patient waiting time. Average MGD and average waiting time was calculated for imaging performed on appropriately matched or mismatched breast size–detector size pairs.
Results
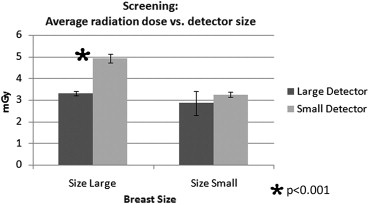
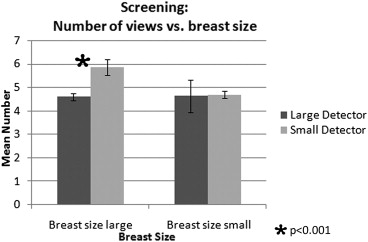
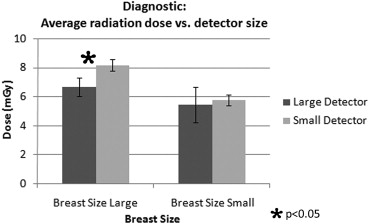
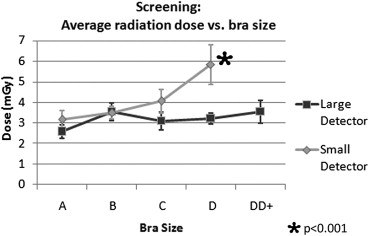
Screening mammography patients with large breasts imaged on a small detector received a significantly higher radiation dose (4.9 vs. 3.3 mGy, P < .05) and a greater number of views (5.9 vs. 4.6, P < .05) compared to optimally matched breast–detector pairs. Dx mammography patients with large breasts imaged on a small detector received a higher radiation dose (8.2 vs. 6.7 mGy, P < .05) compared to optimally matched breast–detector pairs, although without an increased number of views. Waiting times were longer for a large detector.
Conclusions
A mismatch in breast–detector sizes results in a significantly greater radiation dose to patients with large breasts imaged on a small detector. Pressure to minimize patient waiting time may inadvertently result in increased radiation dose. Detector size should be matched to breast size whenever possible, but particularly for patients with larger breast sizes.
The goal of mammography is to identify and evaluate breast cancer and breast disease . The reduction in mortality from breast cancer attributable to screening mammography has been shown to outweigh risks related to radiation exposure . However, in accordance with the general practice mandate of minimizing all diagnostic radiation doses to patients and personnel (the As Low As Reasonably Achievable concept), mammography strives to minimize the examination’s radiation dose. Conventional two-view screening mammography should result in a mean glandular dose per breast on the order of 3–4 mGy . Appropriate imaging should use equipment that minimizes radiation exposure and provides images of diagnostic quality .
Digital mammography has now been routinely integrated into a number of practices, and detectors exist in four basic designs: phosphor-charge coupled devices (CCD), photostimulable phosphors, flat panel phosphors, and selenium flat panel imagers . Each has its benefits and limitations. CCD, the most common type of detector, provides high spatial resolution; however, because of manufacturing constraints CCD-type mammographic detectors are available only in preset sizes (small and large detectors). When using mammographic detectors of different sizes, it is often difficult to match patient breast size to optimal detector size. Our goal was to determine if increased radiation exposure occurs when there is a mismatch between breast size and optimal detector size. To our knowledge, no prior study has evaluated this question.
Materials and methods
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Screening Mammography
Get Radiology Tree app to read full this article<
Diagnostic Mammography
Get Radiology Tree app to read full this article<
Table 1
Mean Age and Number of Patients Imaged with Matched and Mismatched Breast and Detector Size Pairs for Diagnostic and Screening Mammography
Parameter Large Breast Size Small Breast Size Mean age (years) 57.7 55 Screening mammography Number of patients 229 197 Matched 206 143 Mismatched 23 54 Diagnostic mammography Number of patients 161 227 Matched 125 230 Mismatched 36 47
Get Radiology Tree app to read full this article<
Percent Optimally Matched Versus Mismatched
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Radiation Dose
Screening mammography
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Diagnostic mammography
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
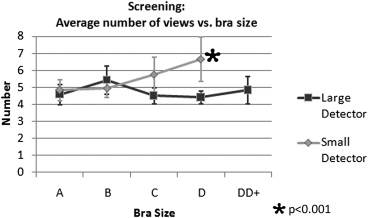
Bra Size
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Waiting Time
Get Radiology Tree app to read full this article<
Patient Positioning with Large Detector
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Conclusion
Get Radiology Tree app to read full this article<
References
1. ACR practice guideline for the performance of screening and diagnostic mammography. Available at: http://www.acr.org/∼/media/3484ca30845348359bad4684779d492d.pdf . Accessed December 15, 2009.
2. Mettler F.A., Upton A.C., Kelsey C.A., et. al.: Benefits versus risks from mammography: a critical reasessment. Cancer 1996; 77: pp. 903-909.
3. Feig S.A., Hendrick R.E.: Radiation risk from screening mammography of women aged 40-49. J Natl Cancer Inst Monogr 1997; 22: pp. 119-124.
4. Yaffe M.J., Mainprize J.G.: Risk of radiation-induced breast cancer from mammographic screening. Radiology 2011; 258: pp. 98-105.
5. Pisano E.D., Yaffe M.J.: Digital mammography. Radiology 2005; 234: pp. 353-362.