
Rationale and Objectives
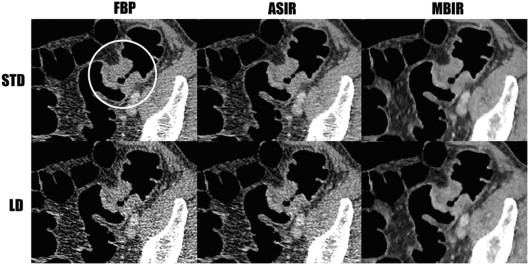
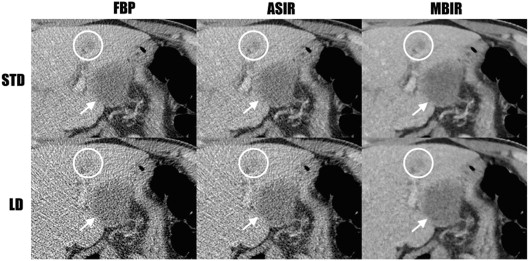
To compare image quality on computed tomographic colonography (CTC) acquired at standard dose (STD) and low dose (LD) using filtered-back projection, adaptive statistical iterative reconstruction, and model-based iterative reconstruction (MBIR) techniques.
Materials and Methods
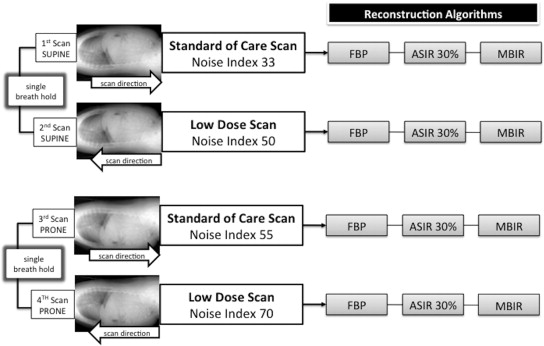
A total of 65 symptomatic patients were prospectively enrolled for the study and underwent STD and LD CTC with filtered-back projection, adaptive statistical iterative reconstruction, and MBIR to allow direct per-patient comparison. Objective image noise, subjective image analyses, and polyp detection were assessed.
Results
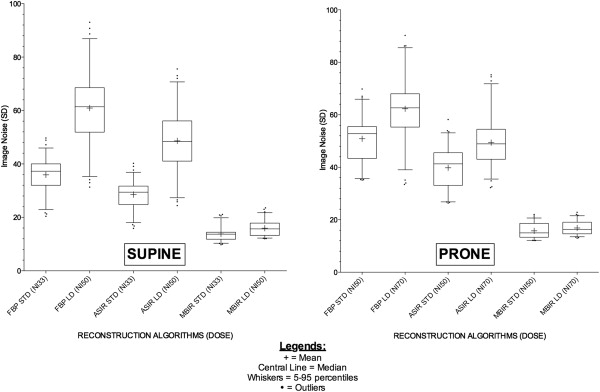
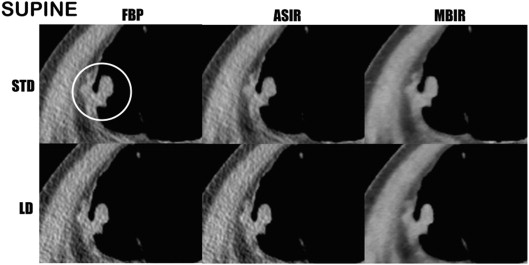
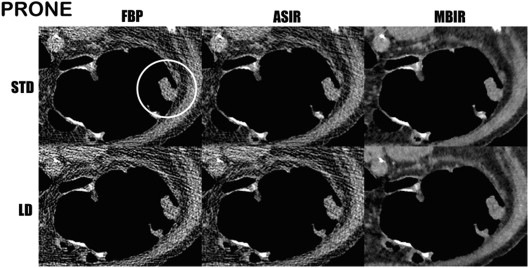
Objective image noise analysis demonstrates significant noise reduction using MBIR technique ( P < .05) despite being acquired at lower doses. Subjective image analyses were superior for LD MBIR in all parameters except visibility of extracolonic lesions (two-dimensional) and visibility of colonic wall (three-dimensional) where there were no significant differences. There was no significant difference in polyp detection rates ( P > .05). Doses: LD (dose-length product, 257.7), STD (dose-length product, 483.6).
Conclusions
LD MBIR CTC objectively shows improved image noise using parameters in our study. Subjectively, image quality is maintained. Polyp detection shows no significant difference but because of small numbers needs further validation. Average dose reduction of 47% can be achieved. This study confirms feasibility of using MBIR in this context of CTC in symptomatic population.
Computed tomographic colonography (CTC) is a widely accepted procedure for the investigation of colorectal cancer, both in the context of symptomatic and screening population . Diagnostic performance has been well validated previously , but the procedure is still associated with high radiation dose especially for symptomatic population with dose estimates of around 7–10 mSv with some studies showing that this trend is not decreasing despite increasing tools available for dose reduction . Using new iterative reconstruction techniques, investigators have performed work on phantom models to assess the accuracy of polyp detection and also there are ongoing clinical trials . Some work has also been performed using other versions of hybrid iterative reconstruction . The aim of our study was to perform low-dose (LD) feasibility study in clinical setting in the symptomatic population. This cohort allows iterative reconstruction to be evaluated on many different levels and for assessment of colonic and extracolonic findings with the methodology allowing direct per-patient comparison of standard-dose (STD) and LD scans based on the findings from previous phantom studies . Our primary objectives were (1) to compare objective image noise between traditional reconstruction method of filtered-back projection (FBP), adaptive statistical iterative reconstruction (ASIR), and model-based iterative reconstruction (MBIR) using STD and LD CT scans; and (2) to compare subjective image noise and quality analysis of STD ASIR scans versus LD MBIR scans to assess feasibility of LD scanning in clinical practice. Our secondary objective was to compare diagnostic accuracy of detected polyps between STD and LD scans across all three reconstruction algorithms.
Materials and methods
Patient Selection
Institutional and regional ethical review board approved this prospectively enrolled study. Informed consent was obtained from all patients. Inclusion criteria were age >50 years, scheduled for a standard-of-care CTC for symptomatic investigation, and fit to undergo the procedure. All patients had standard departmental protocol bowel preparation. Two days before the examination, patient was advised to have low-fiber diet only. The day before the examination, laxatives (sodium picosulfate; Ferring Pharmaceuticals, Saint-Prex, Switzerland) were given as two sachets of 15.08 g dissolved each in one glass of water for morning and afternoon. On the day of examination at 3 hours before examination, Gastrograffin (diatrizoate dimeglumine; Bayer Pharma, Leverkusen, Germany) was given to drink for fecal residue tagging (50 mL in 500 mL of water). Our departmental protocol is in line with the recent European Society of Gastrointestinal and Abdominal Radiology consensus statement . Exclusion criteria included age <50 years, inability to give informed consent, hemodynamic instability, and prior contrast agent reaction. Sixty-five patients were prospectively recruited (26 men and 39 women). Sample size was based on calculation of number that would be needed to reduce mean image noise by a value of 1 (standard deviation (SD) of 1.75) using significance criterion of 0.05 (95% confidence interval) and statistical power of 90%. Referring indications were as follows (and some patients had more than one): weight loss, n = 43; changing bowel habits, n = 34; unexplained anemia, n = 17; abdominal pain, n = 22; palpable mass, n = 13; per rectal bleeding, n = 10; staging scan, n = 8; failed colonoscopy, n = 8; and suspected recurrent disease, n = 5. In terms of prior investigation, other than the eight patients who had failed colonoscopy before this examination, no patients had prior optical colonoscopy or CTC in the preceding 12 months. Mean weight was 75.4 ± 12.1 kg (range, 53–109 kg). Mean age was 75 ± 9.5 years (range, 55–92 years). Scans were performed between October 28, 2012 and March 31, 2013.
Scanning Techniques
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Image Reconstruction
Get Radiology Tree app to read full this article<
Objective Image Noise Analysis
Get Radiology Tree app to read full this article<
Subjective Image Noise and Quality Analysis
Get Radiology Tree app to read full this article<
Polyp Detection
Get Radiology Tree app to read full this article<
Radiation Dose
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Results
Objective Image Noise Analysis
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Subjective Image Noise and Quality Analysis
Get Radiology Tree app to read full this article<
Table 1
Subjective Analysis (Two-Dimensional [2D] Datasets)—Average Scores Between Two Observers
2D Image Noise Visibility of Colonic Wall Overall Diagnostic Confidence Visibility of Extracolonic Lesions Supine Prone Supine Prone Supine Prone Supine Prone ASIR STD MBIR LD ASIR STD MBIR LD ASIR STD MBIR LD ASIR STD MBIR LD ASIR STD MBIR LD ASIR STD MBIR LD ASIR STD MBIR LD ASIR STD MBIR LD Mean 2.2 2 3.1 2.9 2.2 2.1 3.3 3.2 2.1 1.9 2.8 2.7 2.3 2.3 3.3 3.4 SD 0.37 0.26 0.31 0.26 0.38 0.26 0.44 0.44 0.55 0.47 0.81 0.71 0.43 0.42 0.41 0.6 SE 0.046 0.032 0.038 0.033 0.048 0.032 0.055 0.055 0.069 0.059 0.1 0.088 0.054 0.053 0.051 0.074 Lower 95% CI 2.1 1.9 3.1 2.8 2.1 2 3.2 3.1 1.9 1.8 2.6 2.5 2.2 2.2 3.2 3.2 Upper 95% CI 2.3 2.1 3.2 3 2.3 2.1 3.4 3.3 2.2 2 3 2.9 2.4 2.4 3.4 3.5 Kappa 0.891 0.883 0.581 0.633 0.808 0.702 0.725 0.693 0.874 0.881 0.81 0.799 0.814 0.711 0.548 0.73P value 0.0039 0.0003 0.0083 0.0034 0.0027 0.0034 0.3458 0.1983 ∗ ∗ ∗ ∗ ∗ ∗
ASIR, adaptive statistical iterative reconstruction; CI, confidence interval; LD, low dose; MBIR, model-based iterative reconstruction; SE, standard error; SD, standard deviation; STD, standard dose.
Get Radiology Tree app to read full this article<
Table 2
Subjective Analysis (Three-Dimensional [3D] Datasets)—Average Scores Between Two Observers
3D Image Noise Visibility of Colonic Wall Overall Diagnostic Confidence Supine Prone Supine Prone Supine Prone ASIR STD MBIR LD ASIR STD MBIR LD ASIR STD MBIR LD ASIR STD MBIR LD ASIR STD MBIR LD ASIR STD MBIR LD Mean 2.1 2 3.2 2.9 2.1 2.1 3.3 3.3 2.1 2 2.8 2.7 SD 0.34 0.22 0.34 0.32 0.41 0.2 0.43 0.48 0.59 0.54 0.8 0.78 SE 0.042 0.027 0.043 0.04 0.051 0.025 0.053 0.059 0.073 0.067 0.099 0.096 Lower 95% CI 2.1 1.9 3.1 2.8 2 2 3.2 3.1 1.9 1.9 2.6 2.5 Upper 95% CI 2.2 2 3.2 2.9 2.2 2.1 3.4 3.4 2.2 2.1 3 2.9 Kappa 0.871 0.851 0.641 0.572 0.814 0.548 0.814 0.711 0.875 0.901 0.812 0.805P value 0.0054 <0.0001 0.0961 0.1489 0.031 0.0107 ∗ ∗ ∗ ∗
ASIR, adaptive statistical iterative reconstruction; CI, confidence interval; LD, low dose; MBIR, model-based iterative reconstruction; SE, standard error; SD, standard deviation; STD, standard dose.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Polyp Detection
Get Radiology Tree app to read full this article<
Table 3
Per-Polyp Sensitivity, Specificity, PPV, and NPV Between Two Observers
Reconstruction Sensitivity Specificity PPV NPV Reader 1 Reader 2 Reader 1 Reader 2 Reader 1 Reader 2 Reader 1 Reader 2 FBP STD 0.94 0.94 0.88 0.88 0.89 0.89 0.94 0.94 FBP LD 0.82 0.88 0.76 0.82 0.78 0.83 0.81 0.88 ASIR STD 1.00 1.00 1.00 1.00 1.00 1.00 1.00 1.00 ASIR LD 0.94 0.94 1.00 1.00 1.00 1.00 0.94 0.94 MBIR STD 1.00 1.00 1.00 1.00 1.00 1.00 1.00 1.00 MBIR LD 0.94 0.94 1.00 1.00 1.00 1.00 0.94 0.94
ASIR, adaptive statistical iterative reconstruction; FBP, filtered-back projection; LD, low dose; MBIR, model-based iterative reconstruction; NPV, negative predictive value; PPV, positive predictive value; STD, standard dose.
Get Radiology Tree app to read full this article<
Radiation Dose
Get Radiology Tree app to read full this article<
Table 4
Dose-Length Products and Effective Dose for STD and LD Scans
Reconstruction STD LD DLPs (mGy cm) ED ∗ (mSv) DLPs (mGy cm) ED ∗ (mSv) Supine Prone Total Total Supine Prone Total Total Average 346.0 137.6 483.67.3 165.3 92.4 257.73.9 SD 222.3 105.8 129.8 71.9 Range (112.0–1130.0) (23.0–547.3) (27.3–675.0) (15.9–36.48) CTDIs (mGy) CTDIs (mGy) Average 7.05 2.8 3.36 1.88 SD 4.51 2.16 2.63 1.47 Range (2.24–21.4) (0.51–11.3) (0.56–13.97) (0.35–7.63)
CTDIs, computed tomography dose index; DLP, dose-length product; ED, effective dose; LD, low dose; SD, standard deviation; STD, standard dose.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Conclusions
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Atkin W., Dadswell E., Wooldrage K., et. al.: Computed tomographic colonography versus colonoscopy for investigation of patients with symptoms suggestive of colorectal cancer (SIGGAR): a multicentre randomised trial. Lancet 2013; 381: pp. 1194-1202.
2. Almond L.M., Bowley D.M., Karandikar S.S., et. al.: Role of CT colonography in symptomatic assessment, surveillance and screening. Int J Colorectal Dis 2011; 26: pp. 959-966.
3. Hara A.K., Blevins M., Chen M.-H., et. al.: ACRIN CT colonography trial: does reader’s preference for primary two-dimensional versus primary three-dimensional interpretation affect performance?. Radiology 2011; 259: pp. 435-441.
4. Hara A.K., Kuo M.D., Blevins M., et. al.: National CT colonography trial (ACRIN 6664): comparison of three full-laxative bowel preparations in more than 2500 average-risk patients. Am J Roentgenol 2011; 196: pp. 1076-1082.
5. Kim D.H., Pickhardt P.J., Taylor A.J., et. al.: CT colonography versus colonoscopy for the detection of advanced neoplasia. N Engl J Med 2007; 357: pp. 1403-1412.
6. Liedenbaum M.H., Venema H.W., Stoker J.: Radiation dose in CT colonography—trends in time and differences between daily practice and screening protocols. Eur Radiol 2008; 18: pp. 2222-2230.
7. Albert J.M.: Radiation risk from CT: implications for cancer screening. Am J Roentgenol 2013; 201: pp. W81-W87.
8. Boellaard T.N., Venema H.W., Streekstra G.J., et. al.: Effective radiation dose in CT colonography: is there a downward trend?. Acad Radiol 2012; 19: pp. 1127-1133.
9. Yoon M.A., Kim S.H., Lee J.M., et. al.: Adaptive statistical iterative reconstruction and Veo: assessment of image quality and diagnostic performance in CT colonography at various radiation doses. J Comput Assist Tomogr 2012; 36: pp. 596-601.
10. Pickhardt P.J., Lubner M.G., Kim D.H., et. al.: Abdominal CT with model-based iterative reconstruction (MBIR): initial results of a prospective trial comparing ultralow-dose with standard-dose imaging. Am J Roentgenol 2012; 199: pp. 1266-1274.
11. Fletcher J.G., Grant K.L.R., Fidler J.L., et. al.: Validation of dual-source single-tube reconstruction as a method to obtain half-dose images to evaluate radiation dose and noise reduction: phantom and human assessment using CT colonography and sinogram-affirmed iterative reconstruction (SAFIRE). J Comput Assist Tomogr 2012; 36: pp. 560-569.
12. Vardhanabhuti V., Loader R., Roobottom C.A.: Assessment of image quality on effects of varying tube voltage and automatic tube current modulation with hybrid and pure iterative reconstruction techniques in abdominal/pelvic CT: a phantom study. Invest Radiol 2013; 48: pp. 167-174.
13. Neri E., Halligan S., Hellström M., et. al., ESGAR CT Colonography Working Group : The second ESGAR consensus statement on CT colonography. Eur Radiol 2012; 23: pp. 720-729.
14. Deak P.D., Smal Y., Kalender W.A.: Multisection CT protocols: sex- and age-specific conversion factors used to determine effective dose from dose-length product 1. Radiology 2010; 257: pp. 158-166.
15. Miéville F.A., Gudinchet F., Brunelle F., et. al.: Iterative reconstruction methods in two different MDCT scanners: physical metrics and 4-alternative forced-choice detectability experiments—a phantom approach. Phys Med 2013; 29: pp. 99-110.
16. Vardhanabhuti V., Loader R.J., Mitchell G.R., et. al.: Image quality assessment of standard- and low-dose chest CT using filtered back projection, adaptive statistical iterative reconstruction, and novel model-based iterative reconstruction algorithms. Am J Roentgenol 2013; 200: pp. 545-552.
17. Katsura M., Matsuda I., Akahane M., et. al.: Model-based iterative reconstruction technique for ultralow-dose chest CT: comparison of pulmonary nodule detectability with the adaptive statistical iterative reconstruction technique. Invest Radiol 2013; 48: pp. 206.
18. Ichikawa Y., Kitagawa K., Nagasawa N., et. al.: CT of the chest with model-based, fully iterative reconstruction: comparison with adaptive statistical iterative reconstruction. BMC Med Imaging 2013; 13: 1–1
19. Deák Z., Grimm J.M., Treitl M., et. al.: Filtered back projection, adaptive statistical iterative reconstruction, and a model-based iterative reconstruction in abdominal CT: an experimental clinical study. Radiology 2013; 266: pp. 197-206.
20. Yasaka K., Katsura M., Akahane M., et. al.: Model-based iterative reconstruction for reduction of radiation dose in abdominopelvic CT: comparison to adaptive statistical iterative reconstruction. Springerplus 2013; 2: pp. 209.
21. Vardhanabhuti V., Riordan R.D., Mitchell G.R., et. al.: Image comparative assessment using iterative reconstructions: clinical comparison of low-dose abdominal/pelvic computed tomography between adaptive statistical, model-based iterative reconstructions and traditional filtered back projection in 65 patients. Invest Radiol 2014; 49: pp. 209-216.
22. Hansen N.J., Kaza R.K., Maturen K.E., et. al.: Evaluation of low-dose CT angiography with model-based iterative reconstruction after endovascular aneurysm repair of a thoracic or abdominal aortic aneurysm. Am J Roentgenol 2014; 202: pp. 648-655.
23. Pickhardt P.J., Choi J.R., Hwang I., et. al.: Computed tomographic virtual colonoscopy to screen for colorectal neoplasia in asymptomatic adults. N Engl J Med 2003; 349: pp. 2191-2200.
24. Plumb A.A., Halligan S., Taylor S.A., et. al.: CT colonography in the English Bowel Cancer Screening Programme: national survey of current practice. Clin Radiol 2013; 68: pp. 479-487.
25. Levin B., Lieberman D.A., McFarland B., et. al.: Screening and surveillance for the early detection of colorectal cancer and adenomatous polyps, 2008: a joint guideline from the American Cancer Society, the US Multi-Society Task Force on Colorectal Cancer, and the American College of Radiology. CA Cancer J Clin 2008; 58: pp. 130-160.
26. Simons P.C.G., Steenbergen L.N., Witte M.T., et. al.: Miss rate of colorectal cancer at CT colonography in average-risk symptomatic patients. Eur Radiol 2012; 23: pp. 908-913.
27. Spreng A., Netzer P., Mattich J., et. al.: Importance of extracolonic findings at IV contrast medium-enhanced CT colonography versus those at non-enhanced CT colonography. Eur Radiol 2005; 15: pp. 2088-2095.
28. Pickhardt P.J., Hanson M.E., Vanness D.J., et. al.: Unsuspected extracolonic findings at screening CT colonography: clinical and economic impact. Radiology 2008; 249: pp. 151-159.
29. Flicker M.S., Tsoukas A.T., Hazra A., et. al.: Economic impact of extracolonic findings at computed tomographic colonography. J Comput Assist Tomogr 2008; 32: pp. 497-503.
30. Kimberly J.R., Phillips K.C., Santago P., et. al.: Extracolonic findings at virtual colonoscopy: an important consideration in asymptomatic colorectal cancer screening. J Gen Intern Med 2009; 24: pp. 69-73.
31. Pox C.P., Schmiegel W.: Role of CT colonography in colorectal cancer screening: risks and benefits. Gut 2010; 59: pp. 692-700.
32. Park S.H., Lee J.H., Lee S.S., et. al.: CT colonography for detection and characterisation of synchronous proximal colonic lesions in patients with stenosing colorectal cancer. Gut 2012; 61: pp. 1716-1722.
33. Millerd P.J., Paden R.G., Lund J.T., et. al.: Reducing the radiation dose for computed tomography colonography using model-based iterative reconstruction. Abdom Imaging 2014;
34. Graser A., Stieber P., Nagel D., et. al.: Comparison of CT colonography, colonoscopy, sigmoidoscopy and faecal occult blood tests for the detection of advanced adenoma in an average risk population. Gut 2009; 58: pp. 241-248.
35. Flicek K.T., Hara A.K., Silva A.C., et. al.: Reducing the radiation dose for CT colonography using adaptive statistical iterative reconstruction: a pilot study. Am J Roentgenol 2010; 195: pp. 126-131.
36. Chang K.J., Caovan D.B., Grand D.J., et. al.: Reducing radiation dose at CT colonography: decreasing tube voltage to 100 kVp. Radiology 2013; 266: pp. 791-800.
37. Ginsburg M., Obara P., Wise L., et. al.: BMI-based radiation dose reduction in CT colonography. Acad Radiol 2013; 20: pp. 486-492.