
Rationale and Objectives
Severe calcifications of the coronary arteries are still a major challenge in coronary computed tomography (CT) angiography (CCTA). Subtraction CCTA using a 320-detector row CT scanner has recently been introduced for patients with severe calcifications. However, the conventional subtraction CCTA method requires a long breath-holding time of approximately 20–40 seconds. This is a major problem in clinical practice because many patients may not be able to perform such a long breath-hold. We explored a modified subtraction CCTA method with a short breath-holding time to overcome this problem.
Materials and Methods
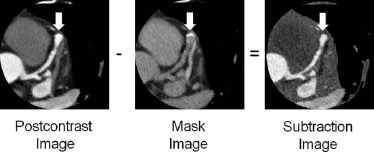
This study was approved by our institutional review board, and all patients gave written informed consent. A total of 12 patients with a coronary calcium score of >400 were enrolled in this study. All patients were unable to hold their breath for more than 20 seconds. Modified subtraction CCTA was performed using the bolus-tracking method. The acquisition protocol was adjusted so that the mask scan was acquired 10 seconds after the postcontrast scan during a single breath-hold. The subtraction image was obtained by subtracting the mask image data from the postcontrast image data. The breath-holding times were recorded. Enhancement of the coronary arteries in the subtraction images was assessed. Subjective image quality was evaluated in a total of 32 segments using a 4-point scale.
Results
The mean breath-holding time was 12.8 ± 0.8 seconds (range, 12–14 seconds). The average CT number in the coronary arteries was 288.6 ± 80.5 Hounsfield units (HU) in the subtraction images. Average image quality was significantly increased from 2.1 ± 0.9 with conventional CCTA to 3.1 ± 0.7 with subtraction CCTA ( P < 0.001). With subtraction CCTA, the number of non-diagnostic segments was significantly reduced from 53% to 19% ( P = 0.001).
Conclusions
This preliminary study has shown that our modified subtraction CCTA method allows the breath-holding time to be shortened to <15 seconds. This may substantially improve the success rate of subtraction CCTA by reducing artifacts and allowing this technique to be applied to patients who are unable to perform a long breath-hold.
Introduction
One of the major challenges in coronary computed tomography (CT) angiography (CCTA) is the presence of severe calcifications in the coronary arteries, which frequently reduces diagnostic accuracy and may even make it impossible to evaluate the presence of stenosis .
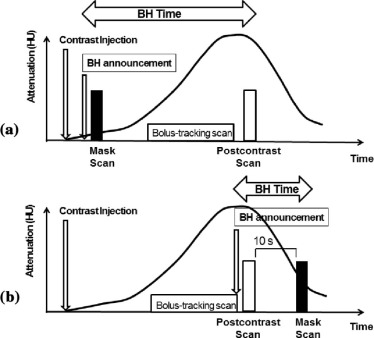
Subtraction CCTA has recently been introduced using first-and second-generation 320-detector row CT technology . In subtraction CCTA, scanning is performed twice to acquire both a precontrast (mask image) and a postcontrast image datasets. To minimize misregistration artifacts due to differences in the breath-hold position, the two scans should preferably be acquired during a single breath-hold . In the conventional subtraction CCTA protocol, the scan for obtaining the mask image (mask scan) is acquired immediately after contrast injection, with the postcontrast scan acquired after the contrast medium has reached the coronary arteries ( Fig 1a ). In this protocol, a long breath-holding time of approximately 20–40 seconds is required between the mask and the postcontrast scans .
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Materials and Methods
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Table 1
Patient Characteristics ( n = 12)
Characteristics Values Age (years) 71.5 ± 7.7 Male ( n ) 5 (42%) Body mass index (kg/m 2 ) 25.4 ± 4.4 Coronary risk factors ( n ) Hypertension 7 (58%) Diabetes 3 (25%) Hypercholesterolemia 6 (50%) Smoking 2 (17%) Previous myocardial infarction 4 (33%) Previous PCI 4 (33%) Coronary calcium score (Agatston score) Range 425.9–1774.7 Mean ± SD 893.3 ± 428.4 HR at postcontrast scan (beats/min) 56.1 ± 10.6 HR at mask scan (beats/min) 56.3 ± 7.9 Use of beta-blockade ( n ) 8 (67%) Estimated effective radiation dose (sum of postcontrast and mask scans, mSv) 5.2 ± 2.2 Breath-holding time (seconds) 12.8 ± 0.8 CT number of coronary arteries (HU) Postcontrast image 397.8 ± 79.9 Mask image 97.8 ± 22.8 Subtraction image 288.6 ± 80.5
CT, computed tomography; HU, Hounsfield units; HR, heart rate; PCI, percutaneous coronary intervention; SD, standard deviation.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Conclusions
Get Radiology Tree app to read full this article<
Acknowledgments
Get Radiology Tree app to read full this article<
References
1. Budoff M.J., Dowe D., Jollis J.G., et. al.: Diagnostic performance of 64-multidetector row coronary computed tomographic angiography for evaluation of coronary artery stenosis in individuals without known coronary artery disease: results from the prospective multicenter ACCURACY (Assessment by Coronary Computed Tomographic Angiography of Individuals Undergoing Invasive Coronary Angiography) trial. J Am Coll Cardiol 2008; 52: pp. 1724-1732.
2. Vavere A.L., Arbab-Zadeh A., Rochitte C.E., et. al.: Coronary artery stenoses: accuracy of 64-detector row CT angiography in segments with mild, moderate, or severe calcification—a subanalysis of the CORE-64 trial. Radiology 2011; 261: pp. 100-108.
3. Abdulla J., Pedersen K.S., Budoff M., et. al.: Influence of coronary calcification on the diagnostic accuracy of 64-slice computed tomography coronary angiography: a systematic review and meta-analysis. Int J Cardiovasc Imaging 2012; 28: pp. 943-953.
4. Yoshioka K., Tanaka R., Muranaka K.: Subtraction coronary CT angiography for calcified lesions. Cardiol Clin 2012; 30: pp. 93-102.
5. Tanaka R., Yoshioka K., Muranaka K., et. al.: Improved evaluation of calcified segments on coronary CT angiography: a feasibility study of coronary calcium subtraction. Int J Cardiovasc Imaging 2013; 29: pp. 75-81.
6. Yoshioka K., Tanaka R., Muranaka K., et. al.: Subtraction coronary CT angiography using second-generation 320-detector row CT. Int J Cardiovasc Imaging 2015; 31: pp. 51-58.
7. Amanuma M., Kondo T., Sno T., et. al.: Subtraction coronary computed tomography in patients with severe calcification. Int J Cardiovasc Imaging 2015; 31: pp. 1635-1642.
8. Cademartiri F., Mollet N.R., Lemos P.A., et. al.: Higher intracoronary attenuation improves diagnostic accuracy in MDCT coronary angiography. AJR Am J Roentgenol 2006; 187: pp. W430-W433.
9. Austen W.G., Edward J.E., Frye R.L., et. al.: A reporting system on patients evaluated for coronary artery disease. Report of the Ad Hoc Committee for Grading of Coronary Artery Disease, Council on Cardiovascular Surgery, American Heart Association. Circulation 1975; 51: pp. 5-40.
10. Meijboom W.B., Meijs M.F., Schuijf J.D., et. al.: Diagnostic accuracy of 64-slice computed tomography coronary angiography: a prospective, multicenter, multivendor study. J Am Coll Cardiol 2008; 52: pp. 2135-2144.
11. Vilades Medel D., Leta R., Alomar Serralach X., et. al.: Reliability of a new method for coronary artery calcium or metal subtraction by 320-row cardiac CT. Eur Radiol 2015; Epub ahead of print
12. Fuchs A., Kuhl J.T., Chen M.Y., et. al.: Feasibility of coronary calcium and stent image subtraction using 320-detector row CT angiography. J Cardiovasc Comput Tomogr 2015; 9: pp. 393-398.
13. Amanuma M., Kondo T., Sano T., et. al.: Assessment of coronary in-stent restenosis: value of subtraction coronary computed tomography angiography. Int J Cardiovasc Imaging 2016; 32: pp. 661-670.
14. Kidoh M., Utsunomiya D., Oda S., et. al.: Optimized subtraction coronary CT angiography protocol for clinical use with short breath-holding time—initial experience. Acad Radiol 2015; 22: pp. 117-120.
15. Abbara S., Arbab-Zadeh A., Callister T.Q., et. al.: SCCT guidelines for performance of coronary computed tomographic angiography: a report of the Society of Cardiovascular Computed Tomography Guidelines Committee. J Cardiovasc Comput Tomogr 2009; 3: pp. 190-204.
16. Huda W., Tipnis S., Sterzik A., et. al.: Computing effective dose in cardiac CT. Phys Med Biol 2010; 55: pp. 3675-3684.