
Rationale and Objectives
The purpose of this study was to optimize photon energy setting to reduce metal artifact of computed tomography (CT) images from implanted metal orthopedic devices in patients with fractures with monoenergetic imaging of dual-energy CT.
Materials and Methods
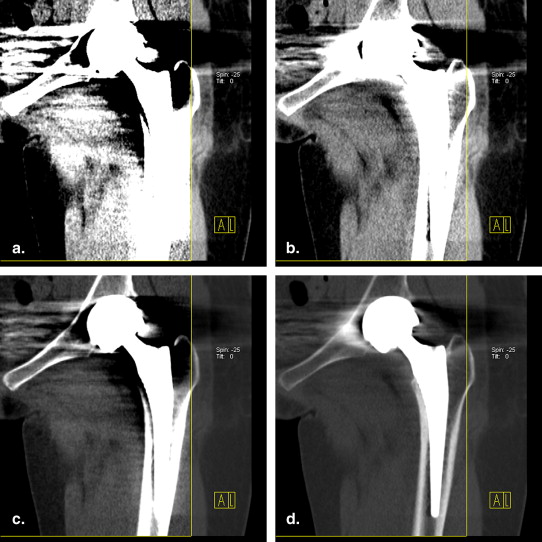
This study included 47 patients with factures who underwent metal orthopedic device implanting. After dual-energy CT scan, monoenergetic software was used to postprocess with the following six photon energies: 40 kiloelectron-voltage (keV), 70 keV, 100 keV, 130 keV, 160 keV, and 190 keV. Two radiologists evaluated and rated the reformatted images with six different photon energies and average weighted 120 kVp images according to 4-score scale. The Wilcoxon rank-sum test was used to compare image quality scores for total, internal, and external metal orthopedic devices. Interreader agreement for image quality scoring was calculated.
Results
Monoenergetic imaging of dual-energy CT improved the quality of CT images in the fracture patients with metal orthopedic devices compared to the average weighted 120 kVp images for the total, external, and internal metal orthopedic devices (all P values < .01). Optimal keV setting with the lowest metal artifact was 130 keV for total, internal, and external metal orthopedic devices. Good interreader agreement was found for the evaluation of image quality for total, internal, and external metal orthopedic devices.
Conclusions
Monoenergetic imaging of dual-energy CT improves quality of CT images in patients with metal orthopedic devices after fracture. Reformatted images at 130 keV have the optimal quality for total, internal, and external metal orthopedic devices.
Multidetector computed tomography (CT) with short scan times and isotropic spatial resolution has been widely used in the preoperative and postoperative evaluation of bony lesions; however, the quality of CT images can still be markedly deteriorated by the presence of metal objects in the field of view. Metal artifacts, mostly from quantum noise, scattered radiation, and beam hardening , influence image quality by reducing contrast and by obscuring details, thus impairing the detectability of structures of interest; in the worst case, this can make a diagnosis impossible . It is, therefore, of great importance to reduce these deteriorating artifacts to a minimum for better diagnosis.
Many authors have recommended using higher milliampere second and peak kilovoltage techniques, the smallest collimator size, soft-tissue reconstruction filters, or extended CT Hounsfield unit scale to decrease CT artifacts arising from metal implants; however, these methods can deliver the patients higher radiation dose or decreased spatial resolution or even unavailable . Although many methods for metal artifact reduction in the raw data have been proposed, most algorithms did not provide sufficient quality to be accepted for clinical application . Methods for metal artifact reduction based on postreconstruction data have rarely been investigated . A dual-energy CT (DECT) technique, one image postprocessing method after image reconstruction , was used to reduce the beam-hardening artifact in CT in the 1980s . However, the dual-energy CT technique has not been used widely for clinical indications because of lower spatial resolution, unstable CT numbers, and insufficient tube currents at low tube voltages of the early CT scanners . Recently developed dual-source CT scanners with two orthogonally mounted detectors and tubes arrays operating simultaneously at different tube potentials (80 kVp and 140 kVp) allow for DECT acquisitions with minimal patient motion registration artifacts and were used to improve the detection of pulmonary embolism and cardiovascular diseases , and to characterize the composition of kidney stones . Herein, we report our preliminary results of the simulated monoenergetic imaging of DECT in reducing the effect of metal artifact on the adjacent bone and soft tissue in 47 patients with implanted metal orthopedic devices after factures.
Materials and methods
Patient Population
Get Radiology Tree app to read full this article<
Table 1
Locations, Numbers, and Types of Metal Implanted Metal Devices in this Study
Locations Internal Implanted metal Device External Implanted Metal Device Total Lower extremity 18 10 28 Upper extremity 7 3 10 Cervical vertebra 9 0 9 Lumbar vertebra 7 0 7
Data presented in this table are numbers of implanted metal devices.
Get Radiology Tree app to read full this article<
Dual-energy CT Imaging
Get Radiology Tree app to read full this article<
Image Postprocessing and Analysis
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Table 2
Comparison of Image Quality of Metal Fixation Among Different Photon Energies ( n )
Score 40 keV 70 keV 100 keV 130 keV 160 keV 190 keV 120 kVp ∗ χ 2 value_P_ Value Total 4 0/0 0/0 16/20 14/14 0/5 2/0 0/0 3 0/0 2/6 29/30 34/39 42/48 41/49 10/13 2 0/0 51/47 9/4 6/1 12/1 11/5 44/41 1 54/54 1/1 0/0 0/0 0/0 0/0 0/0 Rank 28.0/28.0 125.7/119.4 271.4/278.0 276.0/273.4 235.2/254.7 241.4/233.9 148.9/139.2 0.671 <.01 External implanted metal device 4 0/0 0/0 0/0 3/2 0/1 2/0 0/0 3 0/0 0/1 8/13 7/11 10/12 8/11 0/0 2 0/0 13/12 5/0 3/0 3/0 3/2 13/13 1 13/13 0/0 0/0 0/0 0/0 0/0 0/0 Rank 7.0/7.0 33.5/29.9 56.0/64.5 66.0/68.4 61.6/66.5 64.5/58.7 33.5/27.0 0.700 <.01 Internal implanted metal device 4 0/0 0/0 16/20 11/12 0/4 0/0 0/0 3 0/0 2/5 21/17 27/28 32/36 33/38 10/13 2 0/0 38/35 4/4 3/1 9/1 8/3 31/28 1 41/41 1/1 0/0 0/0 0/0 0/0 0/0 Rank 21.5/21.5 92.7/89.9 217.0/215.0 210.4/205.8 174.1/188.9 176.7/175.4 115.6/111.6 0.661 <.01
Get Radiology Tree app to read full this article<

Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Watzke O., Kalender W.A.: A pragmatic approach to metal artifact reduction in CT: merging of metal artifact reduced images. Eur Radiol 2004; 14: pp. 849-856.
2. Kalender W.A., Hebel R., Ebersberger J.: Reduction of CT artifacts caused by metallic implants. Radiology 1987; 164: pp. 576-577.
3. Yazdia M., Gingras L., Beaulieu L.: An adaptive approach to metal artifact reduction in helical computed tomography for radiation therapy treatment planning: experimental and clinical studies. Int J Radiat Oncol Biol Phys 2005; 62: pp. 1224-1231.
4. Liu P.T., Pavlicek W.P., Peter M.B., et. al.: Metal artifact reduction image reconstruction algorithm for CT of implanted metal orthopedic devices: a work in progress. Skeletal Radiol 2009; 38: pp. 797-802.
5. Yu L., Li H., Mueller J., et. al.: Metal artifact reduction from reformatted projections for hip prostheses in multislice helical computed tomography techniques and initial clinical results. Invest Radiol 2009; 44: pp. 691-696.
6. Prell D., Kyriakou Y., Kachelrieß M., et. al.: Reducing metal artifacts in computed tomography caused by hip endoprostheses using a physics-based approach. Invest Radiol 2010; 45: pp. 747-754.
7. Prell D., Kyriakou Y., Struffert T., et. al.: Metal artifact reduction for clipping and coiling in interventional c-arm CT. AJNR Am J Neuroradiol 2010; 31: pp. 634-639.
8. Zhang Y., Zhang L., Zhu X.R., et. al.: Reducing metal artifacts in con-beam CT images by preprocessing projection data. Int J Radiat Oncol Biol Phys 2007; 67: pp. 924-932.
9. Lee M.J., Kim S., Lee S.A., et. al.: Overcoming artifacts from metallic orthopedic implants at high-field-strength MR imaging and multi-detector CT. Radiographics 2007; 27: pp. 791-803.
10. Link T.M., Berning W., Scherf S., et. al.: CT of metal implants: reduction of artifacts using an extended CT scale technique. J Comput Assist Tomogr 2000; 24: pp. 165-172.
11. Hemmingsson A., Jung B., Ytterbergh C.: Dual energy computed tomography: simulated monoenergetic and material-selective imaging. J Comput Assist Tomogr 1986; 10: pp. 490-499.
12. Fletcher J.G., Takahashi N., Hartman R., et. al.: Dual-energy and dual-source CT: is there a role in the abdomen and pelvis. Radiol Clin N Am 2009; 47: pp. 41-57.
13. Johnson T.R., Krauss B., Sedlmair M., et. al.: Material differentiation by dual energy CT: initial experience. Eur Radiol 2007; 17: pp. 1510-1517.
14. Zhang L.J., Zhao Y.E., Wu S.Y., et. al.: Pulmonary embolism detection with dual-energy CT: experimental study of dual-source CT in rabbits. Radiology 2009; 252: pp. 61-70.
15. Zhang L.J., Chai X., Wu S.Y., et. al.: Detection of pulmonary embolism by dual energy CT: correlation with perfusion scintigraphy and pathohistological findings in rabbits. Eur Radiol 2009; 19: pp. 2844-2854.
16. Zhang L.J., Wu S.Y., Niu J.B., et. al.: Dual energy CT angiography for the evaluation of intracranial aneurysms: image quality, radiation dose, and comparison with 3D rotational digital subtraction angiography. AJR Am J Roentgenol 2010; 194: pp. 23-30.
17. Zhang L.J., Peng J., Wu S.Y., et. al.: Dual source dual energy CT of acute myocardial infraction: correlation with histopathological findings in a canine model. Invest Radiol 2010; 45: pp. 290-297.
18. Thomas C., Heuschmid M., Schilling D., et. al.: Urinary calculi composed of uric acid, cystine, and mineral salts: differentiation with dual-energy CT at a radiation dose comparable to that of intravenous pyelography. Radiology 2010; 257: pp. 402-409.
19. Bamberg F., Dierks A., Nikolaou K., et. al.: Metal artifact reduction by dual energy computed tomography using monoenergetic extrapolation. Eur Radiol 2011; 21: pp. 1424-1429.