
Rationale and Objective
The aim of this study was to determine the distinctive features of normal-pressure hydrocephalus (NPH) and other dementias on routine T1-weighted and T2-weighted magnetic resonance (MR) images. Also, the contribution of these parameters to the diagnosis and treatment of NPH was investigated.
Materials and Methods
Routine MR images were used to investigate the morphologic features (dilatation of Sylvian cisterns, narrowness of convexity sulci, thickness of corpus callosum (TCC), and dilatation of perihippocampal fissures) and the flow void phenomenon (FVP) in patients with idiopathic NPH (INPH) and other dementias. Routine MR images of 18 patients with INPH, 11 with dementias other than INPH, and 20 controls were retrospectively examined. Morphologic features and the FVP were graded subjectively. The TCC was measured quantitatively. Morphologic parameters, the FVP, and the shunt response were assessed using Kruskal-Wallis and Mann-Whitney U tests.
Results
The mean FVP score was significantly higher in patients with INPH (2.89 ± 0.75) than in controls and patients with other dementias (1.1 ± 0.85 and 1.09 ± 0.83, respectively) ( P < .001). There was significant difference in terms of TCC between patients with INPH (3 ± 0.7 mm), those with other dementias (1.9 ± 0.7 mm), and controls (5.2 ± 0.8 mm) ( P < .001). Significant differences in terms of other morphologic features were found between patients with INPH and those with other dementias ( P < .05). No significant difference was found between morphologic parameters and the FVP and the outcome of cerebrospinal fluid diversion ( P > .05).
Conclusions
Intense FVP is a signature of but is not pathognomonic for INPH. The morphologic analysis of MR images can be distinctive for the diagnosis of INPH or dementias other than INPH. Detailed evaluation of morphologic features and the FVP in routine MR workup of dementia will be useful for accurate diagnosis.
Normal-pressure hydrocephalus (NPH), a rare disease in the population, is generally seen in the elderly . NPH may be either idiopathic (INPH) or secondary to subarachnoid hemorrhage, meningitis, cranial trauma, and intracranial surgery . INPH is characterized by gait disturbance, dementia, and/or urinary incontinence with normal opening pressure at lumbar puncture in patients without causative disorders, and ventricular enlargement due to disturbed cerebrospinal fluid (CSF) circulation .
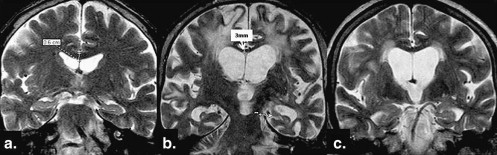
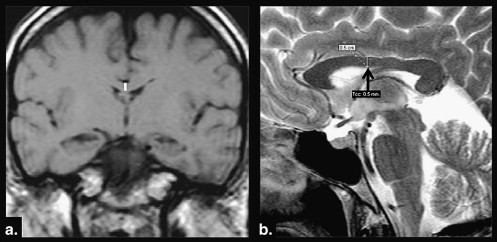
Diagnosis of INPH is of great importance. Because many patients with possibly curable INPH often are misdiagnosed as having Alzheimer’s disease (AD) or vascular dementia, improvement after the temporary removal of CSF and shunt surgery is not always adequately provided . Magnetic resonance imaging (MRI) is an important neuroimaging technique in the diagnosis of INPH. Presence of the flow void phenomenon (FVP) on T2-weighted (T2W) images supports the diagnosis . The degree of the FVP has been reported to correlate with shunt efficacy . Specific morphologic changes, including enlarged Sylvian fissures and tight medial parietal sulci, ventriculomegaly without enlargement of the convexity sulci and perihippocampal fissures (PHFs), and the thickness of the corpus callosum (TCC) on conventional cranial MRI are also useful . Some studies have shown that the FVP and these morphologic magnetic resonance (MR) changes have no additive diagnostic and prognostic value for INPH . As a result of these conflicting results, the value of the FVP and specific morphologic MR changes as diagnostic tests in INPH is uncertain.
Get Radiology Tree app to read full this article<
Materials and methods
Subjects
Get Radiology Tree app to read full this article<
Table 1
Demographic Characteristics of the Groups
Variable Group 1: Patients with INPH Group 2: Patients with Other Dementias Group 3: Controls Number of cases (women/men) 18 (10/8) 11 (5/6) 20 (10/10) Mean age (y) (range) 66 (50–75) 64 (45–79) 53 (40–75)
INPH, idiopathic normal-pressure hydrocephalus.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
MR Procedure
Get Radiology Tree app to read full this article<
Data Analysis
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Table 2
Shunt Outcomes, FVP Scores, and Morphologic Features of Patients with Probable INPH (Group 1)
Patient Sex Age (y) Gait Apraxia Urinary Incontinence Dementia TCC (mm) SWCL SCW Dilatation of PHFs FVP Shunt Outcome 1 F 75 + + + 4 0 2 0 3 + 2 F 63 + + + 3 0 2 0 4 − 3 M 65 + + + 3 1 1 0 3 − 4 M 70 + − + 4 0 2 1 3 + 5 M 66 + + + 2 1 1 1 2 + 6 M 66 + + + 3 1 1 0 2 + 7 F 68 + + + 3 1 1 1 3 + 8 F 50 + − + 3 0 2 0 2 − 9 M 50 + − + 4 1 2 0 3 + 10 F 75 + + + 2 1 2 1 4 + 11 F 70 + − + 3 2 2 1 3 + 12 M 73 + + + 3 2 3 2 2 − 13 M 59 + + + 3 1 2 1 2 − 14 F 60 + + + 2 1 1 1 4 − 15 M 73 + + + 3 0 2 0 3 + 16 F 57 + + + 2 0 3 1 2 + 17 F 74 + + + 4 1 2 1 3 + 18 F 72 + + + 3 1 2 1 4 +
FVP, flow void phenomenon; INPH, idiopathic normal pressure hydrocephalus; PHF, perihippocampal fissure; SCW, Sylvian cistern width; SWCL, sulcal width at convexity level; TCC, thickness of the corpus callosum.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
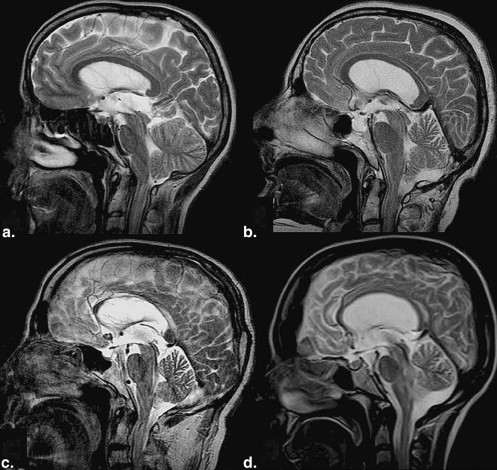
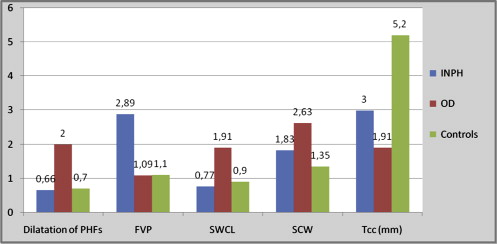
Table 3
Morphologic Characteristics of the Groups
P Value Mean Score NPH Group OD Group Control Group Among Groups NPH vs Control NPH vs OD OD vs. Control Shunt Response FVP 2.89 ± 0.7 1.09 ± 0.8 1.1 ± 0.8 <.001 <.001 <.001 NS NS TCC (mm) 3 ± 0.7 1.91 ± 0.7 5.2 ± 0.8 <.001 <.001 .001 <.001 NS Dilatation of PHFs 0.66 ± 0.6 2 ± 1.09 0.7 ± 0.5 <.001 NS .001 .001 NS SCW 1.83 ± 0.6 2.63 ± 0.7 1.35 ± 0.8 <.001 NS <.05 <.001 NS SWCL 0.77 ± 0.6 1.91 ± 0.7 0.9 ± 0.6 .001 NS .001 <.05 NS
FVP, flow void phenomenon; NPH, normal-pressure hydrocephalus; NS, not significant; PHF, perihippocampal fissure; OD, other dementias; SCW, Sylvian cistern width; SWCL, sulcal width at convexity level; TCC, thickness of the corpus callosum.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Conclusions
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Kitagaki H., Mori E., Ishii K., et. al.: CSF spaces in idiopathic normal pressure hydrocephalus: morphology and volumetry. AJNR Am J Neuroradiol 1998; 19: pp. 1277-1284.
2. Bateman G.A., Levi C.R., Schofield P., et. al.: The pathophysiology of the aqueduct stroke volume in normal pressure hydrocephalus: can co-morbidity with other forms of dementia be excluded?. Neuroradiology 2005; 47: pp. 741-748.
3. Gangemi M., Maiuri F., Buonamassa S., et. al.: Endoscopic third ventriculostomy in idiopathic normal pressure hydrocephalus. Neurosurgery 2004; 55: pp. 129-134.
4. Bradley W.G., Whittemore A.R., Kortman K.E., et. al.: Marked cerebrospinal fluid void: indicator of successful shunt in patients with suspected normal-pressure hydrocephalus. Radiology 1991; 178: pp. 459-466.
5. Kim D.S., Choi J.U., Huh R., et. al.: Quantitative assessment of cerebrospinal fluid hydrodynamics using a phase contrast cine MR image in hydrocephalus. Child Nerv Syst 1999; 15: pp. 461-467.
6. Luetmer P.H., Huston J., Friedman J.A., et. al.: Measurement of cerebrospinal fluid flow at the cerebral aqueduct by use of phase-contrast magnetic resonance imaging: technique validation and utility in diagnosing idiopathic normal pressure hydrocephalus. Neurosurgery 2002; 50: pp. 534-542.
7. Benson D., LeMay M., Patent D., et. al.: Diagnosis of normal pressure hydrocephalus. New Eng J Med 1970; 283: pp. 609-615.
8. Sasaki M., Honda S., Yuasa T., et. al.: Narrow CSF space at high convexity and high midline areas in idiopathic normal pressure hydrocephalus detected by axial and coronal MRI. Neuroradiology 2008; 50: pp. 117-122.
9. Mataro M., Matarin M., Poca M.A., et. al.: Functional and magnetic resonance imaging correlates of corpus callosum in normal pressure hydrocephalus before and after shunting. J Neurol Neurosurg Psychiatry 2007; 78: pp. 395-398.
10. Bradley W.G.: Normal pressure hydrocephalus: new concepts on etiology and diagnosis. AJNR Am J Neuroradiol 2000; 21: pp. 1586-1590.
11. Stein S.C.: Normal-pressure hydrocephalus: an update. Neurosurg Q 2001; 11: pp. 26-35.
12. Kazunari Ishii K., Kanda T., Harada A., et. al.: Clinical impact of the callosal angle in the diagnosis of idiopathic normal pressure hydrocephalus. Eur Radiol 2008; 18: pp. 2678-2683.
13. Savolainen S., Paljarvi L., Vapalahti M.: Prevalence of Alzheimer’s disease in patients investigated for presumed normal pressure hydrocephalus: a clinical and neuropathological study. Acta Neurochir (Wien) 1999; 141: pp. 849-853.
14. Ishikawa M.: Clinical guidelines for idiopathic normal pressure hydrocephalus. Neurol Med Chir 2004; 44: pp. 222-223.
15. Bradley W.C., Scalzo D., Queralt J., et. al.: Normal pressure hydrocephalus: evaluation with cerebrospinal fluid flow measurements at MR Imaging. Radiology 1996; 198: pp. 523-529.
16. Bradley W.G.: Cerebrospinal fluid dynamics and shunt responsiveness in patients with normal-pressure hydrocephalus. Mayo Clin Proc 2002; 77: pp. 507-508.
17. Krauss J.K., Havle B.: Normal pressure hydrocephalus: survey of contemporary diagnostic algorithms and therapeutic decision-making in clinical practice. Acta Neurochir 2004; 146: pp. 379-388.
18. Holodny A.I., Waxman R., George A.E., et. al.: MR differential diagnosis of normal pressure hydrocephalus and Alzheimer disease: significance of perihippocampal fissures. AJNR Am J Neuroradiol 1998; 19: pp. 813-819.
19. Kizu O., Yamada K., Nishimura T.: Proton chemical shift imaging in normal pressure hydrocephalus. AJNR Am J Neuroradiol 2001; 22: pp. 1659-1664.
20. Bateman G.A.: The pathophysiology of idiopathic normal pressure hydrocephalus: cerebral ischemia or altered venous hemodynamics?. AJNR Am J Neuroradiol 2008; 29: pp. 198-203.
21. Brecknell J.E., Brown J.I.M.: Is idiopathic normal pressure hydrocephalus an independent entity?. Acta Neurochir 2004; 146: pp. 1003-1007.
22. Shiino A., Nishida Y., Yasuda H., et. al.: Magnetic resonance spectroscopic determination of a neuronal and axonal marker in white matter predicts reversibility of deficits in secondary normal pressure hydrocephalus. J Neurol Neurosurg Psychiatry 2004; 75: pp. 1141-1148.
23. Hebb A.O., Cusimano M.D.: Idiopathic normal pressure hydrocephalus: a systematic review of diagnosis and outcome. Neurosurgery 2001; 49: pp. 1166-1184.
24. Dixon G.R., Friedman J.A., Luetmer P.H., et. al.: Use of cerebrospinal fluid flow rates measured by phase-contrast MR to predict outcome of ventriculoperitoneal shunting for idiopathic normal pressure hydrocephalus. Mayo Clin Proc 2002; 77: pp. 509-514.
25. Greitz D., Greitz T., Hindmarsh T.: A new view on the CSF-circulation with the potential for pharmalogical treatment of childhood hydrocephalus. Acta Paediatr 1997; 86: pp. 125-132.
26. George A.E., Holodny A., Golomb J., et. al.: The differential diagnosis of Alzheimer’s disease. Cerebral atrophy versus normal pressure hydrocephalus. neuroimaging Clin N Am 1995; 5: pp. 19-31.
27. Li Y., Li J., Segal S., et. al.: Hippocampal cerebrospinal fluid spaces on MR imaging: relationship to aging and Alzheimer disease. AJNR Am J Neuroradiol 2006; 21: pp. 912-918.
28. Lee J.H., Lee H.K., Kim J.K., et. al.: CSF flow quantification of the cerebral aqueduct in normal volunteers using phase contrast cine MR imaging. Korean J Radiol 2004; 5: pp. 81-86.
29. Greitz D., Greitz T.: The pathogenesis and hemodynamics of hydrocephalus. A proposal for a new understanding. Int J Neuroradiol 1997; 3: pp. 367-375.
30. El Sankari S.S., Baledent O., Gondry-Jouet C., et. al.: Aging effects on cerebral blood and cerebrospinal fluid flows. J Cereb Blood Flow Metab 2007; 27: pp. 1563-1572.
31. Kazui H.: Cognitive impairment in patients with idiopathic normal pressure hydrocephalus. Brain Nerve 2008; 60: pp. 225-231.
32. Jack C.R., Mokri B., Laws E.R., et. al.: MR findings in normal-pressure hydrocephalus: significance and comparison with other forms of dementia. J Comput Assist Tomogr 1987; 11: pp. 923-931.
33. Geldmacher D.S., Whitehouse P.J.: Evaluation of dementia. N Engl J Med 1996; 335: pp. 330-336.