
Rationale and Objectives
Previous research has determined that carotid abnormalities (CAs) are partly located >3 cm above the carotid bifurcation. However, identifying CAs occurring in this location using high-frequency linear probes is difficult. The aim of this study was to explore the efficacy of a combination of high-frequency and low-frequency probes in duplex ultrasonography for identifying morphologic features of the internal carotid artery (ICA).
Materials and Methods
A total of 1055 ICAs from 532 patients were analyzed. CAs were classified prospectively according to the criteria of Wain et al, Weibel and Fields, and Metz et al. The diagnostic rates of high-frequency ultrasonography alone and a combination of high-frequency and low-frequency ultrasonography were compared. The distances from the carotid bifurcation to the initial point of the CA and to the mandibular angle were also measured.
Results
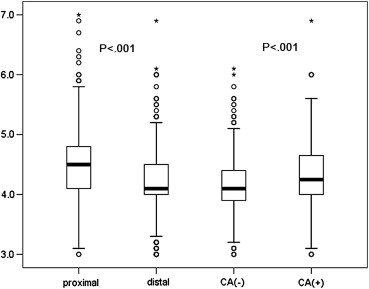
High-frequency ultrasonography detected 23.2% of CAs, and the combination detected 32.2% of CAs ( P < .001) in the 1055 ICAs. Of these CAs, 32.4% and 16.8% began >2.5 and >3 cm above the carotid bifurcation, respectively. The distance between the carotid bifurcation and the mandibular angle was <1.5 cm in 100 arteries (9.48%). The diameter of the distal ICA was larger in patients with CAs than in those without CAs (4.33 ± 0.52 vs 4.13 ± 0.49 mm, P < .001).
Conclusions
Combining high-frequency and low-frequency probes is better than high-frequency probes alone to assess morphologic features of the ICA in duplex ultrasonography. Low-frequency convex probes should be added to traditional ultrasonography for the evaluation of morphologic features of the ICA before carotid endarterectomy, carotid artery stenting, and CA angioplasty.
Carotid endarterectomy (CEA) and carotid artery stenting have become effective means of preventing and treating ischemic stroke, and duplex ultrasonography has been used as noninvasive vascular imaging for screening carotid disease and for identifying candidates for CEA. However, because standard carotid duplex studies describe only the degree and general location of stenotic lesions in the past, only during preoperative angiography can carotid surgeons acquire the necessary anatomic information. On the other hand, carotid abnormalities (CAs) may result in submucosal masses in the posterior pharyngeal wall with clinical symptoms, and these patients can be at risk for surgical injury to the oropharynx and laryngopharynx . Although the incidence and classification of CAs have been reported in many studies using high-frequency linear probes, further improvements are required because some limitations have been reported in high-frequency linear probing, such as incomplete ultrasonography of the internal carotid artery (ICA) in subjects with short conformation of the neck or high bifurcation of the common carotid artery, resulting in exclusion of these subjects from the studies . Herein, we describe a method for improving CA diagnosis rate.
Materials and methods
Pilot Study
In a preliminary study, 64 arteries (excluding two occluded arteries and two arteries with stents) in 34 consecutive patients (22 men, 12 women; mean age, 62.27 ± 10.9 years; range, 40–87 years) were included. Hitachi HI VISION Preirus (Hitachi, Tokyo, Japan) and Toshiba SSA 660A (Toshiba, Tokyo, Japan) color Doppler instruments were used. Frequencies were in the range of 5.5 to 7.5 MHz for the linear-array probe (typically used in carotid studies) and 3.0 to 3.5 MHz for the convex-array probe (typically used in gynecologic studies). The depth of scanning was set at 5 cm for the high-frequency probe and 8 cm for the low-frequency probe. All arteries were scanned in the transverse view followed by the sagittal view. All subjects independently underwent duplex ultrasonography by two sonographers.
Duplex studies
Get Radiology Tree app to read full this article<
ICA classification
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Digital subtraction angiography (DSA)
Get Radiology Tree app to read full this article<
Consistency test
Get Radiology Tree app to read full this article<
General Study
Patients
Get Radiology Tree app to read full this article<
Ultrasound examinations
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Table 1
Comparison between Angiography and Duplex Scanning (Sonographer A) for the Classification of Abnormalities of the Internal Carotid Artery
Duplex Scanning Angiography Total Normal Tortuosity Kinking and Coiling Normal 40 0 0 40 Tortuosity 0 9 3 12 Kinking and coiling 0 2 10 12 Total 40 11 13 64
κ = 0.86, P < .001.
Table 2
Comparison between Sonographer A and Sonographer B for the Classification of Abnormalities of the Internal Carotid Artery
Sonographer A Sonographer B Total Normal Tortuosity Kinking and Coiling Normal 40 0 0 40 Tortuosity 0 10 2 12 Kinking and coiling 0 2 10 12 Total 40 12 12 64
κ = 0.88, P < .001.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
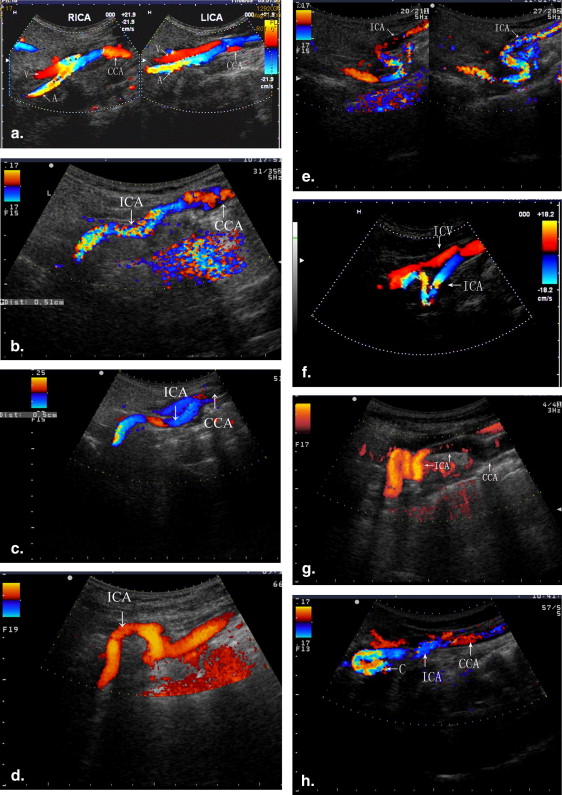
![Figure 4, Comparison of visualization of high-frequency and low-frequency ultrasound. (a) Carotid abnormality of the bilateral internal carotid artery (ICA) was not found using the high-frequency linear probe. (b) In the same patient as in (a) , severe kinking (right ICA [RICA], by color Doppler ultrasound) and coiling (left ICA [LICA], by power Doppler) were fully evident using the low-frequency convex probe, despite occurring at 3.2 cm (RICA) and 3.8 cm (LICA) from the origin of the ICA. (c) Because there was a large acoustic shadow in the proximal ICA, the distal ICA could not be visualized using the high-frequency probe. (d) In the same patient as in (c) , N-shaped moderate kinking was displayed using the low-frequency convex probe. CCA, common carotid artery; LCCA, left common carotid artery; LECA, left external carotid artery. (Color version of figure is available online).](https://storage.googleapis.com/dl.dentistrykey.com/clinical/MorphologicalFeaturesoftheInternalCarotidArtery/3_1s20S1076633212004849.jpg)
Table 3
Distance from the Carotid Bifurcation to the Initial Point of the Carotid Abnormality
Distance From the Bifurcation (cm) Number of Arteries Percentage 0–2.0 137 40.29 2.1–2.5 93 27.35 2.6–3.0 53 15.59 3.1–3.5 29 8.53 3.6–4.0 14 4.12 >4.0 14 4.12 Total 340 100
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 4
Comparison between High-frequency and Combined High-frequency and Low-frequency Ultrasonography for the Diagnosis of CAs
Combination High-frequency Ultrasound Total CA No CA CA 245 95 340 No CA 0 715 715 Total 245 810 1055
CA, carotid abnormality.
χ 2 = 95, P < .001.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Conclusions
Get Radiology Tree app to read full this article<
Acknowledgment
Get Radiology Tree app to read full this article<
References
1. Muñoz A., De Vergas J., Crespo J.: Imaging and clinical findings in patients with aberrant course of the cervical internal carotid arteries. Open Neuroimag J 2010; 4: pp. 174-181.
2. Togay-Işikay C., Kim J., Betterman K., et. al.: Carotid artery tortuosity, kinking, coiling: stroke risk factor, marker, or curiosity?. Acta Neurol Belg 2005; 105: pp. 68-72.
3. Pancera P., Ribul M., Presciuttini B., et. al.: Prevalence of carotid artery kinking in 590 consecutive subjects evaluated by echocolordoppler. Is there a correlation with arterial hypertension?. J Intern Med 2000; 248: pp. 7-12.
4. Wain R.A., Lyon R.T., Veith F.J., et. al.: Accuracy of duplex ultrasound in evaluating carotid artery anatomy before endarterectomy. J Vasc Surg 1998; 27: pp. 235-242.
5. Weibel J., Fields W.S.: Tortuosity, coiling, and kinking of the ICA. Etiology and radiographic anatomy. Neurology 1965; 15: pp. 7-18.
6. Metz H., Murray-Leslie R.M., Bannister R.G., et. al.: Kinking of the ICA in relation to cerebrovascular disease. Lancet 1961; 25: pp. 424-426.
7. Radonic V., Baric D., Giunio L., et. al.: Surgical treatment of kinked internal carotid artery. J Cardiovasc Surg (Torino) 1998; 39: pp. 557-563.
8. Baracchini C., Farina F., Tonello S., et. al.: Endothelial dysfunction in carotid elongation. J Neuroimaging 2011; [Epub ahead of print]
9. Grego F., Lepidi S., Cognolato D., et. al.: Rationale of the surgical treatment of carotid kinking. J Cardiovasc Surg (Torino) 2003; 44: pp. 79-85.
10. Ballotta E., Thiene G., Baracchini C., et. al.: Surgical vs medical treatment for isolated internal carotid artery elongation with coiling or kinking in symptomatic patients: a prospective randomized clinical study. J Vasc Surg 2005; 42: pp. 838-846.
11. Illuminati G., Calió F.G., Papaspyropoulos V., et. al.: Revascularization of the internal carotid artery for isolated, stenotic, and symptomatic kinking. Arch Surg 2003; 138: pp. 192-197.
12. Krings T., Willmes K., Becker R., et. al.: Silent microemboli related to diagnostic cerebral angiography: a matter of operator’s experience and patient’s disease. Neuroradiology 2006; 48: pp. 387-393.
13. AbuRahma A.F., Hayes J.D., Deel J.T., et. al.: Complications of diagnostic carotid/cerebral arteriography when performed by a vascular surgeon. Vasc Endovascular Surg 2006; 40: pp. 189-195.
14. Kaufmann T.J., Huston J., Mandrekar J.N., et. al.: Complications of diagnostic cerebral angiography: evaluation of 19,826 consecutive patients. Radiology 2007; 243: pp. 812-819.
15. Leonardo G., Crescenzi B., Cotrufo R., et. al.: Improvement in accuracy of diagnosis of carotid artery stenosis with duplex ultrasound scanning with combined use of linear array 7.5 MHz and convex array 3.5 MHz probes: validation versus 489 arteriographic procedures. J Vasc Surg 2003; 37: pp. 1240-1247.
16. Hua Y., Liu B.B., Ling C., et. al.: Accurate assessment of the diagnosis between 50-69% and 70-99% carotid stenoses with ultrasonography. Chin J Cerebrovasc Dis 2006; 3: pp. 211-218.
17. Xiong J.Q., Xu E., Li Y.H., et. al.: Ultrasonographic methodology of distal extracranial internal carotid artery and vertebral artery in patient with ischemic encephalopathy. Chin J Ultrasound Diagn 2005; 6: pp. 81-83.
18. Pellegrino L., Prencipe G., Vairo F.: Dolicho-arteriopathies (kinking, coiling, tortuosity) of the carotid arteries: study by color Doppler ultrasonography. Minerva Cardioangiol 1998; 46: pp. 69-76.
19. Krejza J., Arkuszewski M., Kasner S.E., et. al.: Carotid artery diameter in men and women and the relation to body and neck size. Stroke 2006; 37: pp. 1103-1105.