
Rationale and Objectives
This work aimed to quantify the differences in signal-to-noise ratio (SNR) and vessel sharpness between steady-state and first-pass magnetic resonance angiography (MRA) with ferumoxytol in renal transplant recipients.
Materials and Methods
We performed a retrospective study of adult patients who underwent steady-state and first-pass MRA with ferumoxytol to evaluate renal transplant vasculature. SNR was calculated in the external iliac artery, and vessel sharpness was calculated in the external iliac and renal transplant arteries for both acquisitions. Data were compared using Student’s t test.
Results
Fifteen patients were included (mean age 56.9 years, 10 males). The mean SNR of the external iliac artery was 42.2 (SD, 11.9) for the first-pass MRA and 41.8 (SD, 9.7) for the steady-state MRA (p = 0.92). The mean vessel sharpness was significantly higher for the steady-state MRA compared to first-pass MRA for both external iliac (1.24 vs. 0.80 mm −1 , p < 0.01) and renal transplant arteries (1.26 vs. 0.79 mm −1 , p < 0.01).
Conclusion
Steady-state MRA using ferumoxytol improves vessel sharpness while maintaining equivalent SNR compared to conventional first-pass MRA in renal transplant patients.
Introduction
Ferumoxytol is an ultra-small superparamagnetic iron oxide agent used to treat iron-deficiency anemia in patients with renal insufficiency. It causes T1-shortening, and there has been recent interest in its use as a magnetic resonance imaging (MRI) contrast agent . A major advantage of ferumoxytol is its ability to be administered to patients with renal failure. As it is not gadolinium based, there is no risk of nephrogenic systemic fibrosis (NSF). Patients with renal transplants are in a unique position to benefit from this agent. In the setting of graft dysfunction, anatomic imaging of the renal transplant vasculature is often needed to evaluate for transplant renal artery stenosis when ultrasound (US) is inconclusive or intervention is being planned . However, MRI with gadolinium-based contrast agents (GBCAs) and contrast-enhanced computed tomography (CT) are limited by the risks of NSF and contrast-induced nephropathy, respectively.
Ferumoxytol has been preliminarily shown to be useful in evaluating renal transplant arteries in patients with graft dysfunction . This agent is particularly suited for magnetic resonance angiography (MRA) because it initially acts as a blood pool agent that remains in the intravascular space for a prolonged period of time. This allows for steady-state MRA (SS-MRA) to be performed, using prolonged acquisitions that improve signal-to-noise ratio (SNR) and subsequently the potential for improved spatial resolution . In contrast, conventional extracellular GBCAs diffuse into the extravascular space and are rapidly excreted by the kidneys. The intravascular concentration of conventional GBCAs decreases soon after injection, and therefore, MRA is reliant on first-pass arterial phase imaging which limits acquisition time and thus SNR and spatial resolution. Therefore, there is potential for an improvement in image quality using SS-MRA with ferumoxytol compared to conventional first-pass MRA. The purpose of this study is to describe an imaging protocol for SS-MRA with ferumoxytol, and quantify the differences in SNR and vessel sharpness between SS-MRA and first-pass MRA in renal transplant recipients.
Materials and Methods
Patient Population
Get Radiology Tree app to read full this article<
MRI Technique
Get Radiology Tree app to read full this article<
Table 1
Imaging Parameters for First-pass and Steady-state MRA Using Ferumoxytol
First Pass Steady State Field of view 34 cm 26 cm Matrix 320 × 192 384 × 256 Slice thickness 2.8 mm 1.6 mm Spacing 1.4 mm 0.8 mm Mean volume thickness 87 mm 77 mm Voxel size 5.3 mm 3 1.1 mm 3 Nex 1 3 TE 1.6 ms 2.0 ms TR 4.9 ms 6.1 ms Flip angle 30 30 Imaging time 20 s 4.3 min
MRA, magnetic resonance angiography; TE, echo time; TR, repetition time.
Get Radiology Tree app to read full this article<
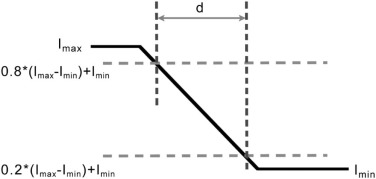
Image Analysis
Get Radiology Tree app to read full this article<
SNR=Sσtot S
N
R
=
S
σ
t
o
t
where S is the mean signal intensity in the iliac artery and σtot σ
t
o
t is the background standard deviation calculated from the six background ROIs using
σtot=(16)(σ12+σ22+…+σ62)−−−−−−−−−−−−−−−−−−−−−−√ σ
t
o
t
=
(
1
6
)
(
σ
1
2
+
σ
2
2
+
…
+
σ
6
2
)
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 2
Mean Edge Sharpness in the External Iliac and Renal Transplant Arteries for First-pass and Steady-state MRA (Numbers in Parentheses are Standard Deviations)
Artery Edge sharpness (mm −1 ) First Pass Steady State p-Value External iliac 0.80 (0.14) 1.22 (0.23) <.01 Renal transplant 0.79 (0.15) 1.26 (0.17) <.01
MRA, magnetic resonance angiography.
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Bashir M.R., Bhatti L., Marin D., et. al.: Emerging applications for ferumoxytol as a contrast agent in MRI. J Magn Reson Imaging 2015; 41: pp. 884-898.
2. Rajan D.K., Stavropoulos S.W., Shlansky-Goldberg R.D.: Management of transplant renal artery stenosis. Semin Intervent Radiol 2004; 21: pp. 259-269.
3. Bashir M.R., Jaffe T.A., Brennan T.V., et. al.: Renal transplant imaging using magnetic resonance angiography with a nonnephrotoxic contrast agent. Transplantation 2013; 96: pp. 91-96.
4. Ruangwattanapaisarn N., Hsiao A., Vasanawala S.S.: Ferumoxytol as an off-label contrast agent in body 3T MR angiography: a pilot study in children. Pediatr Radiol 2014; 45: pp. 831-839.
5. Anzidei M., Napoli A., Marincola B.C., et. al.: Gadofosveset-enhanced MR angiography of carotid arteries: does steady-state imaging improve accuracy of first-pass imaging? Comparison with selective digital subtraction angiography. Radiology 2009; 251: pp. 457-466.
6. Naehle C.P., Kaestner M., Muller A., et. al.: First-pass and steady-state MR angiography of thoracic vasculature in children and adolescents. JACC Cardiovasc Imaging 2010; 3: pp. 504-513.
7. Hope M.D., Hope T.A., Zhu C., et. al.: Vascular imaging with ferumoxytol as a contrast agent. AJR Am J Roentgenol 2015; 205: pp. W366-W373.
8. Browne R.F., Tuite D.J.: Imaging of the renal transplant: comparison of MRI with duplex sonography. Abdom Imaging 2006; 31: pp. 461-482.
9. Steubl D., Papachristou E., Wolf P., et. al.: Doppler-ultrasound measurements in renal allografts depend on the patient’s body position. Vasa 2012; 41: pp. 114-119.
10. Sigovan M., Gasper W., Alley H.F., et. al.: USPIO-enhanced MR angiography of arteriovenous fistulas in patients with renal failure. Radiology 2012; 265: pp. 584-590.
11. Mersa B., Gurkan A., Ozcelik B., et. al.: Anastomosis of accessory arteries via microsurgical technique in renal transplantation. Transplant Proc 2011; 43: pp. 819-821.
12. Fananapazir G., Marin D., Suhocki P.V., et. al.: Vascular artifact mimicking thrombosis on MR imaging using ferumoxytol as a contrast agent in abdominal vascular assessment. J Vasc Interv Radiol 2014; 25: pp. 969-976.
13. Lu M., Cohen M.H., Rieves D., et. al.: FDA report: ferumoxytol for intravenous iron therapy in adult patients with chronic kidney disease. Am J Hematol 2010; 85: pp. 315-319.
14. Santosh S., Podaralla P., Miller B.: Anaphylaxis with elevated serum tryptase after administration of intravenous ferumoxytol. NDT Plus 2010; 3: pp. 341-342.
15. Bultman E.M., Klaers J., Johnson K.M., et. al.: Non-contrast enhanced 3D SSFP MRA of the renal allograft vasculature: a comparison between radial linear combination and Cartesian inflow-weighted acquisitions. Magn Reson Imaging 2014; 32: pp. 190-195.
16. Liu X., Berg N., Sheehan J., et. al.: Renal transplant: nonenhanced renal MR angiography with magnetization-prepared steady-state free precession. Radiology 2009; 251: pp. 535-542.
17. Tang H., Wang Z., Wang L., et. al.: Depiction of transplant renal vascular anatomy and complications: unenhanced MR angiography by using spatial labeling with multiple inversion pulses. Radiology 2014; 271: pp. 879-887.